





Too much meat and dairy and NOT enough B vitamins
Elevated amounts of homocysteine (Hcy) produced from the amino acid methionine in meat and dairy can cause inflammatory damage in several age-related diseases. Hyperhomocysteinemia is shown in osteoporosis, Alzheimer’s disease, Parkinson’s disease, and cardiovascular disease (CVD), and associated with (but not limited to) cancer, aortic aneurism, hypothyroidism, end renal stage disease Damage is caused by inflammatory cytokines to such as collagen and elastin in connective tissue; Kumar et al, 2017- Homocysteine (Hcy) is not DIRECTLY obtained from the diet. Hcy is formed from the metabolism of the essential amino acid, methionine, abundant in red meat and dairy products. Vegetables, with few exceptions (e.g, sesame seeds and Brazil nuts), are low in methionine;
- Adequate amounts of folic acid (B9) and other B vitamins are needed to convert homocysteine into less toxic amino-acids – Vitamin B2 (riboflavin) and magnesium are also involved in homocysteine metabolism.
- Common levels in Western populations are 10 – 12 μmol/L. Levels of 20 μmol/L are found in populations with low B-vitamin intakes or in the older elderly.
- Higher Hcy levels are associated with various health problems. Including cancer, diabetes, CVD, age-related macular degeneration, hearing loss, brain atrophy, dementia, migraine and thyroid disease, prescription drug use, age, declining ability to absorb B12, deteriorating kidney function, smoking, coffee consumption, and excessive alcohol intake, lack of exercise, obesity, stress, and inheriting a variant gene for MTHFR;
- Homocysteine levels can be reduced by:
- Remethylation (~50%) – utilizes active folate (MTHR), B12 and the enzyme MTHFR to convert homocysteine back to methionine. (Also this conversion occurs in kidney and liver via betaine homocysteine methyltransferase (BHMT) which transfers a methyl group to homocysteine via the demethylation of trimethylglycine (TMG / aka betaine, which serves as a methyl donor) to dimethylglycine (DMG)) ;
- Transsulfuration (~50%) – utilizes the active form of vitamin B6 (pyridoxal-5′-phosphate) and the enzyme cystathionine-synthase (CBS). Once formed from cystathionine, cysteine can then be used by the body to make protein and glutathione (GSH), a powerful antioxidant.
If either of these pathways are impaired (E.g. due to a deficiency of B6, B12, folate, betaine), then plasma fasting Hcy concentrations are increased, significantly so in the remethylation pathway.
- Homocysteine (Hcy) levels can be increased by:
- Low thyroid activity – which depletes intracellular magnesium promoting Hcy accumulation. McCully (1983).
- Fluoride, Chlorine, and bromine. These goitrogens lower thyroid activity and thus increase Hcy. Iodine supplementation counters these goitrogens; Yiamouiannis, J.(1986); McCully. K.S. (1983)
- The rare hereditary disease homocystinuria (HCU) elevates Hcy levels. An inherited autosomal recessive trait (both parents carry defective gene) of a disorder of methione metabolism. This can be caused by a deficiency of the enzyme cystathionine-synthase (CBS) or methione synthase, or B6, B9 or B12 deficiency, or those people with a genetic trait, which decreases activity of an enzyme called MTHFR (see inset). MTHFR metabolizes folic acid to its active form; however, a significant reduction in plasma Hcy is achieved by taking an active folate (5-MTHF) supplement.
MTHFRAn enzyme used to produce a substrate involved in the beneficial conversion of Hcy to methionine. A DNA sequence variant (polymorphism) in MTHFR results in its decreased enzymatic activity. This trait is present in about 10% of the world population and it is linked to an increased incidence of thrombosis and CVD, occurring more often in people with above minimal levels of Hcy (~6 μmol/L). |
- Studies indicate that those with Hcy values >or = 6.3 µmol/L are at increased risk of atherosclerosis.
- Women have 10-15% less Hcy during their reproductive decades than men which may help explain the fact they suffer heart attacks on average 10 to 15 years later than men; A practical Hcy goal after age 50 is < 7-8 μmol/L;
- Hcy is associated with higher risk of strokes. Rabelo, 2022
- Hcy is a ‘corrosive’ of the three main structural components of the artery. i.e. the connective tissue proteins collagen, elastin and proteoglycans (e.g. fibrillin is a glycoprotein needed to form elastic fibers). Hcy prevents the formation of stable peptide bonds by tending to cleave to itself.
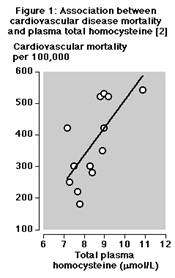
Credit for Figure 1: G Alfthan et al, Plasma homocysteine and cardiovascular disease mortality. Lancet 1997
- Even slightly elevated Hcy level promotes tiny clots that initiate arterial damage and large clots that precipitate heart attacks and strokes. Gibson et al, 1964; Morin et al, 1991; Editorial, 1981
- Baboons infused with Hcy for 5-30 days developed arterial damage proportion to Hcy concentration. There was no correlation to cholesterol. Harker et al, 1974.
- Men with high Hcy levels had > 3 times more heart attacks than those with low Hcy levels
- Men with 3 clogged coronary arteries had higher Hcy than men with 1. Malinow MR. 1989; Stampfer et al, 1992
- Anti-atherogenic, anti-clotting benefit of fish oil may result from lowering Hcy. Olszewski AJ et al, 1993;
- Cholesterol is oxidized by Hcy to generate oxysterols (oxygenated derivatives of cholesterol) and arterial damage is proportional to the concentration of oxysterols (LDL cholesterol is only an accomplice to arterial damage through oxidative modification). Hcy also generates oxysterols in food exposed to high heat and oxygen. E.g powdered egg yolk or milk, gelatin (Hcy is the only dietary substance to do so, other than damaged fatty acids,such as trans fatty acids). Processed foods may increase oxysterol presence 1000 times higher than normal.
- Long-term vitamin B6 supplementation protects against heart problems. in 1950, Dr. Moses M. Suzman (neurologist/internist) in S. Africa started his patients on a daily dose of 100 mg B6, before they were diagnosed with heart problems. Over the course of 44 years, Dr. Suzman could not point to a single one of his tens of thousands of patients who had had a coronary spasm, cardiac arrest or stroke, and “far fewer cardiac problems than would have been expected.”In 1969, he changed the daily dose to 200 mg B6 (half as a complex) and 600 IU vitamin E. In 1972, he also added vitamin C, selenium, magnesium and other nutrients;
- Common in pregnancy
- Many peoples’ livers can not convert B6 supplement pyridoxine hydrochloride to pyridoxal phosphate (PLP) – the active form of B6 in the body.
- Consequence of methionine-rich high-animal protein diets and high dietary sugar;
- Vitamin B6 seems to protect against oxysterols – B6 has been found by several researchers to act as an antioxidant in high enough concentration, protecting against oxysterols









