
Pregnancy issues and how to deal with them

Journey of an egg - "From follicle to uterus"
The beginning
A woman has two almond-shaped and sized ovaries (one each side of the uterus). They take turns each monthly cycle to produce and develop eggs (ova) for fertilization.
The egg journey begins in an ovarian follicle. As many as a dozen follicles, which are egg-containing, ¼-1″ diameter cyst-like sacs filled with fluid and hormones (mostly estrogen), start to ripen within an ovary during the first 14 days of the menstrual cycle (which begins day 1 of the monthly period). One or two of these follicles grow stronger than the others, producing and maturing an egg. When ovulation is triggered by a surge in LUTEINIZING HORMONE (LH), the dominant follicle ruptures, releasing its egg into the fallopian tube en route to the uterus, where either the egg is fertilized by a sperm within 24 hours, or it dies.
The now empty follicle egg sac in the ovary becomes a corpus luteum, producing and secreting ESTRADIOL and PROGESTERONE to prepare and provide support for a possible pregnancy. PROGESTERONE is produced from yellow, fatty cholesterol in the corpus luteum, which is Latin for “yellow body”. It’s pro-gestational functions include:
- Thicken the uterine lining (endometrium) to a max. 4-6 mm
- Aid secretion of nutrients from endometrial glands
Stimulate secretion of immune system Th2 and reduce secretion of Th1 cytokines. To prevent mother’s immune system from responding to fetal antigens and rejecting the newly arrived “foreign body” 🙂
If conception occurs
Under the influence of HUMAN CHORIONIC GONADOTROPIN (hCG ) from a developing embryo – the corpus luteum ovarian granulosa cells produce large amounts (25-50 mg/day) of PROGESTERONE and smaller amounts (0.5mg/day) of ESTRADIOL) crucial for the first 10 weeks of gestation (counted from day 1 of last mentrual period) Csapo, 1973, at which time the placenta is usually able to produce sufficient PROGESTERONE to support the pregnancy. Insufficient PROGESTERONE at this so-called luteal phase can prevent conception or cause miscarriage, which can be remedied by providing supplemental PROGESTERONE
Conception Problems or Miscarriage related to luteal phase deficiency (LPD)
The fertilized egg undergoes rapid cell division and implants on the prepared uterine wall 5-6 days after ovulation. hCG must appear 4 days after ovulation to rescue the Corpus luteum from regression. Corpus luteum has a negligible role in 2nd and 3rd trimesters.
At term gestation,the placenta produces about 250 mg PROGESTERONE / day and PROGESTERONE levels range from 100-200 ng/ml.
If conception does NOT occur
Without any hCG influence from an embryo, then about 10 days after ovulation, the corpus luteum usually disintegrates (via a process called luteolysis). Next, the uterine lining is shed (seen as menstrual bleeding),
Do's and Don'ts of pregnancy
Folate (B9) and cobalamin (B12) are essential for pregnancy
Folate deficiency in expectant mother can produce a neural tube defect (NTD) in her fus at around 3 weeks after conception.
- A neural tube defect (NTD) is the most common birth defect – occurs in ~ 1 in 1,000 U.S. live births results from a folate deficiency affecting the neural tube in the developing fetus. The top part of the neural tube forms the baby’s brain and the bottom part unfolds to become the baby’s spinal column.An opening in the spinal cord or brain occurs very early in human development and normally fuses to form the neural tube around the 3rd week of pregnancy. An NTD develops when the neural tube does not close completely, resulting in serious brain and spinal problems. NTDS include: anencephaly, encephaloceles, hydranencephaly, iniencephaly, schizencephaly, and spina bifida..
- An NTD occurs on days 27-29 after conception (i.e. before many women are even aware they are pregnant) – thus not allowing an opportunity after conception to raise the mother’s (and therefore the newly-conceived infant’s) folate levels to reduce NTD risk .
- Sufficient folate (vitamin B9) and its cofactor vitamin B12 reduce NTD occurrences, since folate is required for production and maintenance of new cells, for DNA synthesis and RNA synthesis. Molloy et al, 2009
- Vitamin B12 is an important receptor in the folate synthesis pathway and studies have shown that vitamin B12 deficiency contributes to risk of NTDs. Li et al, 2009
If pregnancy is a possibility, ensure you have adequate folate levels. Every woman who has any chance at all of becoming pregnant should:
- Ensure folate sources in your diet – particularly green vegetables, beans, peas, brewer’s yeast, and liver (only organic).
- Take a folate supplement together with its cofactor vitamin B12 (methylcobalamin form). It is important that these supplements are in the natural form i.e folinic acid or 5-MTHF, and not labeled folic acid or folate, which are both synthetic forms
Neutrophilic Hypersegmentation Index (NHI) test for folate status. If you are planning or have any chance of becoming pregnant,this inexpensive blood test can confirm your folate levels. With a low folate test result, a woman should immediately have a series of folate injections; For anyone else, ensure your diet contains sufficient folate.
For details on folate and the NHI test, see:
Avoid fluoride ==> Pre-term births / Anemia
Avoiding fluoride reduces anemia, pre-term and low-weight babies
“Anemic pregnant women living in India, whose urine contained 1 mg/L fluoride or more, were separated into two groups. The experimental group avoided fluoride in water, food and other sources …
Results reveal that anemia was reduced and pre-term and low-birth-weight babies were considerably fewer in the fluoride-avoidance group.”
- In the US, researchers from the State University of New York also reported that premature births were more common in communities with fluoridated drinking water than those with non-fluoridated water.
- High fluoride levels seem to damage the gastrointestinal mucosa – leading to impaired nutrient absorption and related problems:
- Anemia (decreased red blood cells) – in pregnancy, this can result in both maternal and infant mortality; anemia persists even with the currently advised maternal iron and folic acid supplementation.
- Reduced blood folic acid activity
- Inhibition of vitamin B12 production
- Non-absorption of nutrients for hemoglobin synthesis
For information on the many other toxic effects of fluoride and the fraudulent studies used to support its addition to community drinking water, see:
Fluoride -Mega Health Fraud / Cover-up
- Fluoridated water – ~80% of the fluoride can be removed from your drinking water using a reverse osmosis (RO) filter.
- Fluoridated toothpaste and mouth rinses
- Food and beverages processed with fluoridated water
- Mechanically de-boned meat
- Pesticide residue on food
- Pharmaceutical drugs – especially SSRI antidepressants and antibiotics fluoroquinolone antibiotics like Cipro and penicillin
- Soy baby formulas
Umbilical cord should not be clamped prematurely- To avoid possible infant brain damage
In 1801, Erasmus Darwin (Charles Darwin’s grandfather) gave us some wise insight on this subject:
“Another thing very injurious to the child, is the tying and cutting of the navel string too soon; which should always be left till the child has not only repeatedly breathed but till all pulsation in the cord ceases. As otherwise the child is much weaker than it ought to be, a portion of the blood being left in the placenta, which ought to have been in the child.”
Cutting the Cord – When a baby is born, one of the first procedures performed is the clamping and cutting of the umbilical cord. A newborn’s lungs are in a “compacted state” whilst still in the womb, however, when the infant is born, the placenta and cord pulse for up to 20 minutes, delivering a burst of blood volume to the infant’s system, necessary for the lungs to expand.llus, luctus nec ullamcorper mattis, pulvinar dapibus leo.

Unfortunately, many hospitals and doctors are clamping the umbilical cord too soon, often within one minute of birth. Since they believe it will reduce the mother’s risk of excess bleeding and the baby’s risk of jaundice. Often cords are also clamped early to collect cord blood and cord stem cells to be used for medical and commercial purposes.
Research is revealing that clamping the umbilical cord before two or three full minutes have elapsed, robs your baby of much-needed blood and oxygen. Without the burst of blood from the placenta, the infant’s blood pressure drops as its lungs fail to open as they should, creating a chain reaction of effects that can include brain and lung damage. One of the primary arguments for delaying cord clamping has to do with the way a baby breathes just before and after being born.
Dr. Mercola explains a baby’s First Breaths in Detail. From his article “Are Doctors Causing Infant Brain Damage by Clamping the Umbilical Cord Prematurely?
“Before birth, the baby’s lungs are filled with fluid and very little blood flows through them; the child receives oxygen from its mother through the placenta and cord. This placental oxygen supply continues after the child is born until the lungs are working and supplying oxygen — that is, when they are filled with air and all the blood from the right side of the heart is flowing through them.
After birth, when the child is crying and pink, the cord vessels clamp themselves. During this interval between birth and natural clamping, blood is transfused from the placenta to establish blood flow through the baby’s lungs. The natural process protects the baby’s brain by providing a continuous oxygen supply from two sources until the second source is functioning well.
However, according to George M. Morley, M.B., Ch. B., FACOG, immediate cord clamping at birth instantly cuts off the placental oxygen supply and the baby remains asphyxiated until the lungs function. Blood, which normally would have been transfused to establish the child’s lung circulation, remains clamped in the placenta, and the child diverts blood from all other organs to fill the lung blood vessels.
While most full-term babies have enough blood to establish lung function and prevent brain damage, the process often leaves them pale and weak. For premature babies, the process can be even more devastating. And no matter what, immediate cord clamping will cause some degree of asphyxia and loss of blood volume, because it:
- Completely cuts off the infant brain’s oxygen supply from the placenta before lungs begin to function
- Stops placental transfusion. The transfer of a large volume of blood (up to 50% increase in total blood volume) that is used mainly to establish circulation through the baby’s lungs to start them functioning.”
Possible Problems resulting from Premature Cord Clamping. Premature clamping of the umbilical cord increases the baby’s risk of brain hemorrhage and breathing problems. It has been implicated as a contributing factor in:
- Hypotension / Hypovolemia (Low blood pressure /volume)
- Autism
- Cerebral Palsy
- Anemia -with resultant cognitive deficits
- Learning disorders and mental deficiency
- Behavioral disorders
- Respiratory distress
- Death (as a result of brain injuries)
Pregnancy-related problems
Morning sickness
What is morning sickness?
- This not so delightful “Joy of Motherhood” has symptoms, not necessarily confined to the morning – include nausea, vomiting, fatigue, lightheadedness, and dizziness during the early stages of pregnancy. Women with morning sickness may be particularly sensitive to certain odors and foods.
- On a positive note – recent studies have suggested that mothers who have morning sickness have fewer miscarriages;
- More severe form with excessive nausea and vomiting is called Hyperemesis Gravidarum
Causes of Morning Sickness?
- No one knows for sure what causes morning sickness – but it is probably a combination of rapidly increasing estrogen and Progesterone levels, an enhanced sense of smell and excess stomach acids.
- One theory is that Progesterone (the dominant hormone during pregnancy) is to blame – Progesterone has a “relaxing” effect on the muscles in the body, preventing preterm labor by effecting the uterine muscles. However, it also effects other muscles, such as the stomach and intestines. The Progesterone relaxes the workings of the whole digestive track which makes the elimination of bodily wastes slower, leading to slower stomach-emptying, causing excess stomach acids.
- Another more popular theory is that morning sickness is caused by the buildup of hCG (human chorionic gonadotopin) – hCG is produced after implantation takes place and continues to increase until about the 12th week of your pregnancy, at which point the levels of hCG starts to decrease. For many women, but not all, this is also when your morning sickness symptoms will start to decrease.
- Women with a high intake of saturated fat during the year prior to pregnancy had a much higher risk of severe morning sickness – than did women eating less saturated fat, according to a Harvard University study. An increase in saturated fat intake of 15 grams per day (E.g. a four-ounce cheeseburger or 3 cups of whole milk) was associated with a greater than threefold increase in the risk of developing morning sickness. Signorello et al, 1996
What can you do to curb morning sickness?
Long and short, there is no one tried and true method that will relieve everyone’s case of morning sickness. However, here are some ideas to try that have worked for others going through the same ordeal:
- Vitamin B6 (pyridoxine). The results of two double-blind, placebo-controlled trials that used B6 suggest that vitamin B6 may be beneficial in alleviating morning sickness – Each study found a slight but significant reduction in nausea or vomiting in pregnant women:
- 25 mg of B6 every eight hours for three days (Vitamin B6 is effective therapy for nausea and vomiting of pregnancy: a randomized, double-blind placebo-controlled study. )
- or 10 mg of B6 every eight hours for five days (Pyridoxine for nausea and vomiting of pregnancy: a randomized, double-blind, placebo-controlled trial).
- Ginger. In 250 mg. capsules 3x daily can be beneficial. Ginger has long been associated with alleviating nausea. A review of six double-blind trials concluded that ginger is probably an effective treatment for nausea and vomiting in pregnancy. (Borelli et al, 2005)
Ginger Tea Recipe |
Peel the ginger root and slice it into thin slices. Bring the water to a boil in a saucepan. |
- “Morning sickness Magic” is a herbal remedy containing Ginger, Vitamin B6, Red Raspberry Leaf and Folic Acid (B9).
- Avoid heat
- Get enough sleep at night / Take naps during the day (but not right after eating) -tiredness plays a big part in morning sickness.
- Get out of bed slowly in the morning
- Eat plain crackers or dry cereal before you get out of bed in the morning
- Open windows / turn on exhaust fans when cooking and after meals – to avoid nausea-promoting smells.
- Carry a handkerchief with a few drops lemon essential oil to breathe – when you can’t get away from a smell that is bothering you.
- Avoid greasy or spicy foods – often cause nausea or heartburn.
- Follow your cravings – they will not lead you the wrong way.
- Have frequent protein snacks – Low fat meats and seafood, nuts, eggs and beans.
- Eat smaller meals every two hours or so – keeps blood sugar levels even; eat meals high in protein and complex carbohydrates.
- Eat something salty before a meal
- Drink liquids and eat solid foods at separate times – do not drink fluids with your meals.
- Drink non caffeinated peppermint and ginger tea
- Avoid dehydration – drink small amounts of fluids regularly though the day.
- Do not skip meals
- Cold food may have less nausea inducing smells associated with them
- Utilize acupressure – or wear a Sea-band, a small band to put pressure on the inner wrist. Acupoint 12 – On the largest crease of the inner wrist, on a line with the thumb, approximately three finger widths up from your hand. See: How to apply acupressure, using Acupoint 12.

- Meridian Tapping Technique – MTT;
- Ensure good liver function nausea is worse if liver not removing toxins and excess hormones from the blood. During the first trimester there is a surge in the production of three major hormones: estrogen, Progesterone, and HCG. The liver is responsible for breaking down the excess hormones produced during pregnancy.
Vitamin C and Vitamin K stimulate detoxifying enzymes in the liver. Vitamins B6 and B12 also help the liver to perform optimally.
- Foods specifically high in Vitamin C include: citrus fruits; lemons, limes, oranges,* strawberries, tomatoes, honeydew, melons, sweet potatoes, green peppers, potatoes.
- Foods high in both Vitamin C and Vitamin K include: broccoli, kale,cauliflower, bok choy, brussel sprouts, cabbage, wheatgrass.
Hyperemesis Gravidarum (HG) (Severe morning sickness)
HG involves excessive nausea and vomiting
One to three percent of pregnant women suffer from an EXCESSIVE amount of nausea and vomiting that interfere with nutrition and hydration. You should consult a qualified medical professional if you are vomiting more than three times a day, are unable to retain any fluids you drink, and are progressively losing weight. HG can be devastating for the mother and detrimental to the baby when the mother is unable to keep anything down and has to be hospitalized for intravenous feeding.
Symptoms
Check your own symptoms against this list as a general indication you are dealing with HG:
Severe and persistent vomiting
Dehydration – signs of dehydration listed below:
- Ketones in urine (easy to test yourself with Ketostix – available online)
- Decreased blood pressure
- Increased heart rate
- Pinched skin returns slowly.
- Flushed dry skin
- Dry eyes
- Dry Mouth
- Coated tongue
- Trouble thinking clearly/confusion
- Decreased urination
- Dark urine
- Loss of weight (anything over 5% of your pre-pregnancy weight)
- Tachycardia (rapid heartbeat)
- Constipation
- Difficulty eating and drinking
- Extreme fatigue
- Nausea aggravated by physical temperature extremes
- Increase in saliva resulting in difficult swallowing
- Slow or inpaired thinking
- Decrease in attentionspan
- Blood electrolyte levels abnormal
- Decreased Motivation
- Decreased physical performance
- Increased anxiety
- Symptoms aggravated by motions
- Poor skin tone
- Dry, shrunken tongue
- Need for intravenous nutrition
- Aching eyeballs, difficulty focusing, rapid vision changes
- Boredom
Evidence suggests that the hormone LEPTIN plays a role in severe morning sickness (and PCOS)
Zofran for HG?
Used for HG, many women have found prescription Zofran (Ondansetron hydrochloride) effective at helping them stay nourished and hydrated
- Zofran is an antiemetic – effective at stopping nausea and vomiting;
- Zofran works by blocking the hormone SEROTONIN – which causes vomiting. Zofran is a selective serotonin-3 (5HT-3) antagonist – 5HT-3 receptors are mainly found in the small intestine (and in the CNS to a lesser degree). By blocking this receptor you decrease the nausea. The 5HT-3 receptor is responsible for the nausea (seen as a start-up side effect of the SSRIs). Stimulation of the 5HT-3 receptor by the increased SEROTONIN (as a result of the SSRI) causes nausea, which is resolved when this receptor is desensitized (usually within the first month after starting the SSRI).
Zofran Safety?
- The FDA labels Zofran as a category B. Given to medicines that have NOT been studied in pregnant humans, but do not appear to cause harm to the fetus in animal studies.
- There are no adequate and well-controlled studies in pregnant women, and therefore this drug should be used during pregnancy only if clearly needed. Studies on pregnant rats and rabbits given Zofran have revealed no evidence of impaired fertility or harm to the fetus.
Possible Side Effects of Zofran
(official Zofran site: http://us.gsk.com/products/assets/us_zofran_tablets.pdf)
- Headache
- Diarrhea
- Constipation
- Fever
- Malaise/fatigue
- Lightheadedness
- Drowsiness
Precautions for Taking Zofran
- Do not drive while taking Zofran
- A history of any of the following problems may affect your being able to take Zofran
- Stomach / intestinal problems
- Liver disease
- Allergies
Save Money BY Buying Generic Zofran. Zofran (Ondansetron hydrochloride) is mega-expensive (~$900 for 30 tablets). Many insurance companies will not cover the cost of Zofran. Ask your doctor for the generic brand of ondansetron, which is much cheaper.
Alternative drugs for nausea
- Emitrol (no prescription needed)
- Bendectin. A combination of Vitamin B6 (pyridoxine) and an antihistamine, doxylamine (antihistamines calm the labyrinthine inner ear); Available in Canada as Dicletin or you can buy the ingredients separately and combine them); FDA declared “Safe and effective for nausea and vomiting of pregnancy.”Compazine (Prochlorperazine) and Phenergan (Promethazine) – these are phenothiazine-like drugs, meaning they act centrally in the brain to relieve nausea. Technically, they’re sedative-antihistamines, like the doxylamine in Bendectin.
Sore nipples from breast-feeding
The best cure is prevention
Getting sore, cracked nipples is a common problem for nursing mothers –The following tactics have helped many mothers avoid suffering from the pain of sore nipples.
Position the baby properly
The baby should be a little bit up from horizontal – and turned so that his / her chest, belly and thighs are against you with a slight tilt so the baby can look at you. You can use a pillow to help support him or her in this position. The baby should approach the breast with the head just slightly tilted backwards, which results in the nipple automatically pointing to the roof of the baby’s mouth.
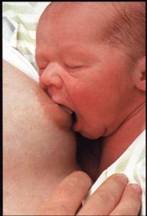
Ensure a good “Latch on”
- The baby should latch on with a wide open mouth covering as much of the areola as possible – Lightly run your nipple along the baby’s upper lip from one corner of the baby’s mouth to the other until his/her mouth is wide open – that is the moment for him or her to latch on.Bring the baby toward the breast such that his or her chinis the first to touch your breast. The nipple points to the roof of the mouth, not the middle of the mouth.
- A properly latched on baby will be covering more of the areola with his/her lower lip than with the upper lip – The baby’s lips should be everted (see picture left).
- You should not be feeling any pain. If the baby is latched on and sucking correctly.
- Do not allow the baby to suck on just the nipple. i.e. with the mouth not covering most of the areola. Use your forefinger next to the corner of the baby’s mouth to break the suction, and have the baby latch on again properly. A good “latch on”also reduces the possibility of the baby getting “gas”, and allows the baby to better control the flow of milk.
Sun-tan the Nipples
Expose your nipples to full sun for 30 minutes / day

Healing cracked / Sore Nipples

Pure Lanolin
Preferably 100% pure, anhydrous, fragrance-free, pharmaceutical grade lanolin (extracted from sheep’s wool). A small amount goes a long way. Gently rub on the nipples between feeds. Wipe off any excess lanolin remaining just before feeding.
Example: Australian Lanolin for Sale at Amazon.com
Some other good brands:Pur-LanTM or LansinohTM
Saline Soak
Mix 1 tsp. salt in 1 cup of warm water in a small bowl. Soak the sore nipple(s) in this solution for 5-10 minutes and then allow to air-dry.
Sea Buckthorn berry oil
Sea buckthorn oil is the MVP for healing skin problems. For most benefit, use organic, cold-pressed oil from the sea buckthorn berry. It costs around $25 for 2oz., but that should be more than enough to deal with the problem. This treatment is also excellent if the soreness is due to thrush, where the baby has a white fungus lining the inside of the mouth. Rub the oil on your nipples and inside the baby’s mouth. It’s perfectly safe – some people take this oil as a health-supplement.

Air the nipples as much as possible / Use breast shells / Avoid direct contact with nursing pads
When airing is not possible, plastic dome-shaped breast shells(not nipple shields) can be worn to protect your nipples from rubbing on your clothing. Nursing pads keep moisture against the nipple and tend to stick to damaged nipples. If you leak a lot you can wear the pad over the breast shell

Nipple shields
A teat is placed over the nipple to enable the baby to suck on the breast without direct contact. However, most mothers have NOT found these to be very helpful.Also, they tend to reduce the milk supply, and once the baby is used to it, he/she may not want to return to the breast.
Herbal remedies
Comfrey ointment. Softens and strengthens nipples. Soothes /heals sensitive nipples.
Yarrow leaf poultices / yarrow infused oil. Provide almost instantaneous pain relief and heal cracked nipples rapidly.
- Fresh aloe vera leaf gel. Soothes/heals heal sore and cracked nipples.
- Calendula ointment. An old favorite to heal and strengthen nipples.
Pospartum depression (PPD)
PPD is a mood disorder affecting ~10-15% of women after childbirth. Experiencing some depression is not uncommon, but usually doesn’t last for > 2 weeks. Symptoms of PPD usually begin between 2 weeks and a month after childbirth. The symptoms involve emotional, behavioral changes and differences in brain activity from women who are not postpartum.
The cause may may be related to estradiol and progesterone levels that increase in pregnancy then fall drastically postpartum within 24 hours. As estradiol falls, so does the neurotransmitter Serotonin, which regulates mood. Obviously, the many lifestyle changes, overwhelming stresses, lack of sleep, financial worries that arrive with a new baby are also factors that increase anxiety and depression.
Dr. Dalton, author of “Guide to Progesterone for Post-Natal Depression”, states that:
“At delivery of the baby, the placenta (which produces Progesterone) is also delivered, and there is a sudden alteration in the levels of all hormones. The new mother must abruptly adjust to the complete absence of Progesterone after nine months of continuous and plentiful supply. It is suggested that some women find this alteration of Progesterone difficult to tolerate and react with the development of postnatal depression.”
NATURAL (bio-identical), not synthetic, Progesterone supplementation may prevent anxiety and other postnatal symptoms and may even be combined with other prescribed medication. Synthetic versions of allopregnanolone have been utilized with some success. Progesterone is being studied as a potential treatment of PPD, but as yet no dose hase been determined, and an insufficient dose may exacerbate the problem.
References
Borrelli F et al (2005) Effectiveness and safety of ginger in the treatment of pregnancy-induced nausea and vomiting. Obstet Gynecol;105:849-56.
Csapo AL, Pulkkinen MO, Wiest WG. (Mar 1973) Effects of luteectomy and progesterone replacement in early pregnant patients. Am J Obstet Gynecol. 115:759. PubMed
Li, F.; Watkins, D.; Rosenblatt, D. S. (2009). “Vitamin B-12 and birth defects”. Molecular Genetics and Metabolism 98(1-2): 166-172.
Molloy, A. M.; Kirke, P. N.; Troendle, J. F.; Burke, H.; Sutton, M.; Brody, L. C.; Scott, JM; Mills, JL (2009). “Maternal Vitamin B-12 Status and Risk of Neural Tube Defects in a Population With High Neural Tube Defect Prevalence and No Folic Acid Fortification. [Article]“. Pediatrics 123(3): 917-923.
Pratap Kumar, Navneet Magon. (2012) Hormones in Pregnancy Niger Med. J. Oct-Dec; 53(4): 179-183 PubMed
Signorello LB et al, (1996) Saturated fat intake and the risk of severe hyperemesis gravidarum. Am J Epidemiol;143 (11 Suppl):S25 [abstract # 97]










