
Clostridium difficile Infection (CDI) - Resulting from overuse of antibiotics
Overview of C. difficile infection
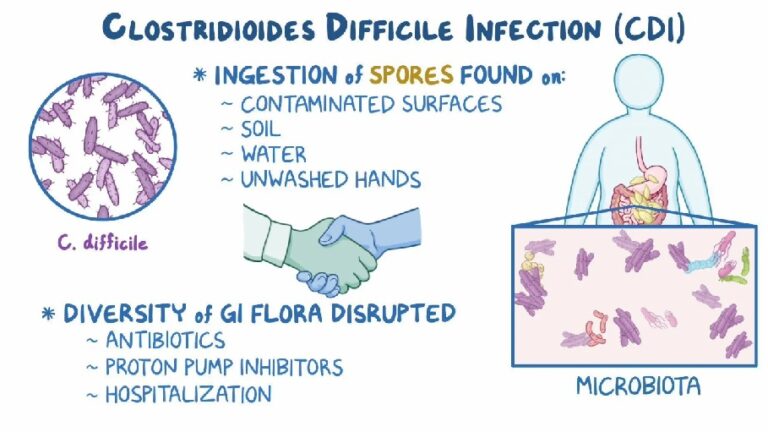
C. difficile is an antibiotic-resistant, toxin-producing bacteria that can infect the intestines. C. difficile infection (CDI) is the most common hospital-acquired infection, occurring as a result of its accidental ingestion. CDI is adding significantly to U.S. hospitalization costs ($6.3bn – in 2016). Gupta A and Ananthakrishnan AN, 2021 Traditionally acquired in a healthcare facility, such as a hospital, nursing home, assisted-living or similar facility, but 2023 CDC data shows around half of cases are originating in the community.
After beneficial, infection-controlling flora have been wiped out or disrupted by a broad-spectrum antibiotic (e.g. penicillins, cephalosporins, clindamycin, fluoroquinolones) or possibly from using proton pump inhibitors (PPIs), C. difficile overruns the normal gut flora (most often in immuno-compromised / elderly patients) and can wreak havoc in the intestines causing damage, inflammation and severe diarrhea.
C. difficile is an anaerobic, gram positive, spore-forming bacterium. Its overpopulation releases toxins (Toxin A and Toxin B) that damage / inflame the lining of the intestines, causing bloating and severe C. difficile-associated diarrhea (CDAD) with abdominal pain. The toxins destroy the normal colon cells and produce pseudo membranes (visualized on colonoscopy as yellowish-white plaques of inflammatory cells on the interior surface of the colon), which can lead to infection of the colon identified as C. difficile colitis or Pseudomembranous colitis, promoting severe inflammation.
CDAD is a major cause of morbidity, especially in the elderly. C. difficile infections (CDIs) have dramatically increased in recent years, with 500,000 cases and ~15,000 deaths annually in the U.S. U.S. Centers for Disease Control & Prevention. A compromised immune system and delayed diagnosis appear to be factors in an elevated risk of death.
Clostridia bacteria are normally found in small amounts in the small intestine ileum and colon. It is rarely found in the oropharynx, stomach, or small intestine’s jejunum.
C. difficile infection is sometimes misdiagnosed as irritable bowel syndrome (IBS) or the stomach flu.
Signs and symptoms of Clostridium Difficile infection
Watery / foul-smelling diarrhea – 3 or more stools per day for 2 or more days
Moderate to severe abdominal cramping and pain
Nausea
Fever
Blood or pus in the stool
Dehydration
Loss of appetite
Weight loss
In severe cases. C. difficile can lead to life threatening complications such as toxic megacolon, peritonitis (inflammation of the abdominal cavity lining), perforation of the colon, sepsis, and death.
Symptoms of recurrent C difficile infection. Shown to involve more severe illness, abdominal pain, and fever than with initial infection
How does someone get contaminated with Clostridium difficile?
DIrect or indirect contact
- C. difficile can be acquired from a carrier and spread by direct or indirect contact. E.g. with contaminated surfaces or hands or air-borne spores. The spores are commonly spread from one patient to another via: (1) Unwashed hands of caregivers or (2) Tubal insertions into the body (E.g. via nasogastric tubes or administration of enemas /enteral feedings).
- The heat-resistant spores can survive outside the body and remain viable for weeks on surfaces. E.g. bed rails, blood pressure cuffs, thermometers, tabletops, telephones, stethoscopes etc. The organism can persist in hospital rooms for up to 40 days after infected patients have been discharged. Hurley BW, Nguyen CC. The spectrum of pseudomembranous enterocolitis and antibiotic-associated diarrhea. Arch Intern Med. 2002;162:2177-84. Another source says C. Diff can survive 5 months even on a dry surface. Kramer A, et al. BMC Infect Dis 2006;6:130 The many spores formed by C. difficile resist most surface cleaning methods. However, here are cleaning solutions that will “get ’em”.
Antibiotic / Other medication involvement in C. Difficile infection
- Broad spectrum antibiotics (E.g. clindamycin, (Cleocin), fluoroquinolones: ciprofloxacin (Cipro) and levofloxacin (Levaquin), cephalosporins: Ceftin, Omnicef, Rocephin, Maxipime) are more strongly associated with C. difficile infections than other antibiotics
- Increasing rates of community-acquired (nosocomial) C. difficile infection are associated with the use of medication that suppress gastric acid production
- H2-receptor antagonists increased the risk 1.5 fold, and proton pump inhibitors by 1.7 with once daily use and 2.4 with more than once daily use.
- All anticholinergic drugs (E.g. the PPI Omeprazole) slow digestive transit time, and so retain toxins to exacerbate gut damage.
- Use of steroid drugs, acid blockers, birth control pills

Other causes include:
- Poor diet, chlorinated water, pesticides
- Decreased immune function , diabetes, hypothyroidism, alcoholism, AIDS, Cancer, and chronic stress
How to treat Clostridium difficile
Discontinue antibiotics and administer fluids /electrolytes
This therapy alone resolves diarrhea in 15-23% of otherwise healthy adults. Schroeder M. Clostridium difficile-associated diarrhea. March 2005. American Academy of Family Physicians Web site
- Discontinue antibiotics
- Drink plenty of water. To keep well hydrated
- Replace electrolytes (potassium, sodium, chloride, bicarbonate). Especially helpful are salty soups for sodium, and bananas (or other fruits/veggies) or tomato juice to replace potassium.
Home remedy: Mix and drink 1/4 tsp. salt, 1/4 tsp. baking soda, 1/2 cup orange juice, 2 tbsp. sugar and 1 liter of water). Also eat a banana or some watermelon for additional potassium.
Treat Clostridium difficile using natural pathogen killers in place of medical antibiotics
- Turmeric (active ingredient: curcumin). 40 U.S. studies are looking at turmeric as a potential inhibitor of C difficile. A turmeric enema may equal vancomycin for C. difficile colitis. Dr. Rattan Patel and his research team found that growth of all strains of C. Difficile was inhibited (in vitro) by extracts of regular grocery store turmeric, at concentrations that would be easily obtained in the colon by adding the spice to food or consuming it in capsule form. Taken orally for therapeutic use, you would need a high quality extract. Dr. Patel maintains that 4 g/day of curcumin achieves a concentration of curcumin in the stool well above the concentrations that inhibited C. difficile growth.
Mercola.com offers a quality curcumin extract
- Iodine. Will kill C-difficile spores.
- Grapefruit seed extract (GSE)
Grapefruit Seed Extract -“Medicine Chest in a Bottle”
- Wild Oregano Oil (WOO)
Probiotics effective at shortening duration of intestinal C. difficile infection
Inhibition of Clostridium difficile strains by intestinal Lactobacillus species and bifidi bacterium species (both lactic acid bacteria) or Saccharomyces species (yeast) (E.g. S. boulardii (Florastor®)) has been clinically shown to shorten the duration of diarrhea.
How do probiotics work against C. difficile (and other pathogens)?
- Antagonistic / Competitive towards pathogenic bacteria
- Stimulate immune mechanisms of intestinal mucosa
Probiotic Supplements.
Take a dose of the highest quality supplemental probiotic you can find – it is generally agreed that:
- A significant number of microorganisms must be consumed in order to alter the bacterial population in the gut
- Several different species of bacteria given simultaneously are preferable to using just one species.
Be aware that many products:
- Contain way too few CFU to amount to a “hill of beans”
- Contain less live microorganisms than claimed on their label
- Contain significantly less live microorganisms than on their production date
Some notable probiotic supplement choices to fight C. difficile:
- VSL # 3® – contains 450 billion live bacteria per dose;
- Dr. Mercola® Complete Probiotics -high production quality, 70 billion CFU / dose, 10 strains of lactobacillus and bifidobacterium.
- Culturelle® (LGG) – 10 billion CFU Lactobacillus rhamnosus strain GG (LGG) + 245g of prebiotic inulin / capsule dose; Vitacost.com. Good survival rate in stomach/bile acid.
- Florastor® -sometimes recommended by doctors but only contains 5 billion CFU / capsule of Saccharomyces boulardii ; Some complain of stomach rumblings.
Ensure probiotic supplement is taken at least 2 hours away from taking antibiotics (E.g. Flagyl or Vancocin). Otherwise the antibiotics will destroy too many of the probiotic bacteria;
For more detail on probiotics, see:
For probiotic dosage suggestions against C. difficile:
Antibiotic / Probiotic Therapy Dosages against C. Difficile Infection
Food sources of probiotics
Kefir. This probiotic liquid contains almost 20 strains of lactobacilli and is used against C. Diff
Dosage. 1/2 cup of kefir four times the first day, then 1/4 cup four times a day for about a week. Can make kefir at home or buy ready-to-eat in a grocery store (in the yogurt section) in plain or flavored. Diluting it with water or juice helps it down.
| Resolution of Recurrent Clostridium difficile-associated Diarrhea Using Staggered Antibiotic Withdrawal and Kefir |
|---|
– By Johan S. Bakken, M. D. , Ph. D. Abstract “Eight patients, each of whom experienced recurrent episodes of Clostridium difficile-associated diarrhea, were treated with staggered and tapered oral metronidazole or vancomycin combined with daily intake of kefir, an over-the-counter liquid probiotic dairy product. All eight successfully resolved their infection and did not experience any further diarrhea after completion of treatment. Further studies will be needed to determine whether gradual antibiotic withdrawal combined with kefir is a valuable treatment for recurrent C. Difficile-associated diarrhea.” |
Yogurt with active cultures. E.g. Stoneyfield, Dannon. Avoid sweetened yogurt, since sugar is food for pathogenic bacteria.
“Cultured cabbage” or “Kimchi” (one recipe includes Chinese cabbage, green onions and ginger root)
Prebiotics (food for probiotics). Research suggests that prebiotics, such as fructooligosaccharides (FOS), may have a role in prevention and treatment of C. difficile infections by helping to restore normal indigenous microflora. These naturally occurring, non-digestible food components are fermented in the colon, having these benefits:
- Selectively utilized by beneficial/probiotic bacteria already in the colon to promote their growth and colonization – thereby having a role in preventing/treating C. difficile infections.
- Normalize bowel function – may be used to manage diarrhea and constipation
| Effect of the prebiotic oligofructose on relapse of Clostridium difficile-associated diarrhea: a randomized, controlled study. |
|---|
We set out to determine if the prebiotic oligofructose could alter the fecal bacterial flora and, in addition to antibiotic treatment, reduce the rate of relapse from C difficile infection. Consecutive inpatients with C difficile-associated diarrhea (CDAD) were randomly allocated to receive oligofructose or placebo for 30 days in addition to specific antibiotic treatment. Patients were followed up for an additional 30 days. The main end point was the development of further diarrhea. Stools were collected for bacterial culture and C difficile toxin measurement. Fecal cultures confirmed the prebiotic effect of oligofructose. Patients taking oligofructose were less likely to develop further diarrhea than those taking the placebo. Clin Gastroenterol Hepatol. 2005. Department of Medicine, Derriford Hospital, Plymouth, UK |
- Fructooligosaccharides (FOS) are the major class of prebiotics. Found in chicory, garlic, onion, wheat, rye, bananas, leeks, tomatoes and honey. Other prebiotics include inulin and oligolactulose.
Other adjunct treatments for Clostridium difficile
Build immune system – E.g. by regularly eating garlic and onions, plus take daily probiotics;
Anti-diarrhea and opiate pain medicines should be avoided. Aince these medications reduce intestinal motility, and stopping diarrhea could cause an already inflamed colon to retain C. Difficile toxins. Better natural options to control diarrhea, would be:
- Consume 2 ripe bananas and a glass of organic buttermilk every day
- Coconut (milk, oil or flakes). Take 1 Tbsp Extra Virgin Coconut Oil or 2 Tbsp. unsweetened, shredded coconut (from health food store), drink coconut milk, or some people have simply eaten supermarket coconut macaroons, but these contain a lot of sugar
A child’s dose of bovine colostrum
Activated charcoal or bentonite clay taken orally will adsorb C. Diff toxins – it is thought that by binding the toxins produced by C. difficile, they will be removed faster from the intestine, causing less damage. However, such adsorbers should not be eaten three hours before or after taking antibiotics or other medications,because it will interfere with their effective natural digestion, and so weaken medication.
Minimize sugar intake. Unless you want to feed the little C. Difficiles !
Recurrence of Clostridium difficile
Occur in ~20% of cases – usually within 2 months after stopping antibiotics for CDAD;
Usually due to reinfection or germination of spores in colon;
Who is likely to have C. difficile recurrence?
- Females
- Patients who have one recurrence – 65% more likely to have further recurrences;
Prevent Clostridium difficile re-infection
Isolate patient from other high-risk persons. This includes other patients, the elderly /immuno-compromised, or those taking antibiotics.
Exercise stringent hand-washing for patient and patient caregivers
Kill C. difficile (including its spores) on hospital or home surfaces.
To kill Clostridium difficile (including its spores) wipe down surfaces (incl. door handles, knobs, toilet seat/ handles, phones, computer and mouse) with any of the following effective solutions:
- 10 parts water to 1 part bleach
- 3% Hydrogen peroxide
- 95% isopropyl alcohol (rubbing alcohol)
- 70% ethanol
- 10% Povidine iodine (Betadyne)
C. difficile and the Environment: Disinfection Practices and Mitigating Risk to Patients
Certain probiotic strains have been shown to prevent antibiotic-associated diarrhea (AAD). There is strong evidence of efficacy for S. boulardii or L. rhamnosus GG in adults or children who are receiving antibiotic therapy. Also, recent research has indicated that L. casei DN-114 001 is effective in hospitalized adult patients for preventing antibiotic-associated and C. difficile diarrhea.
| Some recommended Adult Dosages for Prevention of C Difficile Antibiotic-associated diarrhea (CDAD) | ||
|---|---|---|
| World Gastroenterology | Williams NT. Probiotics | |
L. casei DN-114 001 in fermented milk with L. bulgaricus + S. thermophilus | 10 billion CFU twice daily | |
L. acidophilus + B. bifidum (Cultech strains) | 20 billion CFU each, once daily | |
S. cerevisiae (boulardii) lyo | 20 billion CFU/day | 4 – 20 billion CFU daily for ‘1-4 weeks |
Oligofructose | 4 g / three times/day | |
Lactobacillus rhamnosus strain GG (LGG) | 6 -40 billion CFU daily for 1-2 weeks | |
L acidophilus and L bulgaricus | 2 billion CFU daily for 5-10 days | |
L acidophilus and Bifidobacterium longum | 5 billion CFU daily for 7 days | |
L acidophilus and B lactis | 100 billion CFU daily for 21 days | |
Williams NT. Probiotics. Am J Health-Syst Pharm. 2010;67:449-458.
Lactobacillus rhamnosus strain GG (LGG) (ATCC 53103). US patent 4,839,281, named after it’s co-discoverers, Sherwood Gorbach and Barry Goldin, was identified as the result of a screening effort that evaluated dozens of strains of lactobacilli to identify those with a certain set of desireable probiotic attributes, namely:
- Stability to effects of bile
- Stability to affects of acid
- Ability to attach avidly to mucosal cells of the human intestinal tract
- Lactic acid production
- Hardy growth in vitro
LGG is available in the US as “Culturelle”, which is marketed by CAG Functional Foods and can be bought online.
Gorbach SL, Chang TW, Goldin B.Successful treatment of relapsing Clostridium difficile colitis with lactobacillus GG. (Letter) Lancet 1987;2(8574):1519
Saccharomyces boulardii. Numerous studies have shown S.boulardii an effective treatment for active C.difficile diarrhea. Qamar A. Aboudola S, Warny M, et al.Saccharomyces boulardii stimulates intestinal immunoglobulin A immune response to Clostridium difficile toxin A in mice.Infect Immun.2001; 69:2672-2765
- A non-disease causing yeast;
- Survives passage through the intestinal tract;
- Unaffected by antibiotics – although it can be killed by antifungal medication;
- Disrupts toxins that would normally irritate the intestines – stimulates the intestinal immune system to secrete C. difficile toxin A-specific antibodies (IgA) in the gut.
Lactobacillus acidophilus and Lactobacillus casei proprietary blend (50 billion CFU / capsule) reduced AAD / CDAD in those taking antibiotics. A 2010 study involved 225 hospitalized patients taking antibiotics considered high-risk for C. difficile. Randomly assigned to one of 3 groups, patients took dosages of probiotic blend or placebo (as shown in chart below), begun 36 hours after starting antibiotic course and continued for 5 days after course was finished. Affect on antibiotic-associated diarrhea (AAD) or C. difficile-associated diarrhea (CDAD) was recorded, showing favorable dose-related results for those taking probiotic blend, compared to those taking placebo. Even those patients who experienced AAD on probiotics, had symptoms for a shorter duration than those on placebo.
| L. acidophilus / L. casei proprietary blend was effective for reducing AAD and CDAD in those taking high-risk antibiotics | |||
|---|---|---|---|
| Group | # of capsules | # of CFU | % experiencing ADD or CDAD |
| Placebo | 2 capsules | 0 | 24% |
| Low dose proprietary probiotic blend | 1 capsule | 50 billion | 10% |
| High-dose proprietary probiotic blend | 2 capsules | 100 billion | 1.2% |
Miller et al, Dose-Response Efficacy of a Proprietary Probiotic Formula of Lactobacillus acidophilus CL1285 and Lactobacillus casei LBC80R for Antibiotic-Associated Diarrhea and Clostridium difficile-associated Diarrhea Prophylaxis in Adult Patients, Am. J. of Gastroenterology, Published online ahead of print, doi:10.1038/ajg. 2010.11
Conventional treatment for C. difficile
Antibiotics for Clostridium difficile
There are two mainstream antibiotic choices (however, due to both antibiotic resistance and tactics employed by bacteria for self-protection, these antibiotics may NOT be successful). Also, these antibiotics deal with the active (vegetative) form of C. difficile, but do not kill its spores – which can germinate and possibly “hide” in intestinal folds; Fekety R. Guidelines for the diagnosis and management of Clostridium difficile-associated diarrhea and colitis. Am J Gastroenterol 1997;92(5):739-50
Metronidazole (Flagyl) – usually first choice (several hundred $$$ cheaper and antibiotic resistance less of a concern); destroys functioning enzymes of C. difficile.
Vancomycin (Vancocin HCl) – a bacteriostatic/doesn’t kill bacteria; prevents C. difficile from reproducing.
- The standard antibiotic dose schedule is 4 times a day for 10-14 days. Response to therapy can be assessed by the resolution of fever, usually within the first two days. Diarrhea should improve within 2-4 days and resolve within 2 weeks. .
- Pulse dose antibiotic therapy – involves alternating antibiotic treatment with no medication, each for several days at a time. The theory is that by stopping and starting the antibiotic, the C. difficile spores hatch, and are then killed by the next pulse of antibiotics.
- Tapering off vancomycin or metronidazole over 4-6 weeks may be more effective than stopping abruptly – the theory being that this allows for restoration of normal gut flora whilst antibiotic continues to kill C. difficile.
Joyce AM, Burns DL. Recurrent Clostridium difficile colitis: tackling a tenacious nosocomial infection. Tedesco FJ, Gordon D, Forston WC. Approach to patients with multiple relapses of antibiotic-associated pseudomembranous colitis. Am J Gastroenterol 1985;80(11):867-8
Antibiotic / Probiotic Therapy Dosages for Clostridium difficile
| Standard oral therapy for Clostridum difficile infection | |
|---|---|
| Metronidazole (Flagyl) | 250-500 mg 3 or 4 times daily X 10-14 days |
| If unsuccessful, then Vancomycin (Vancocin, Vancoled) | 125 mg 4 times daily X 10-14 days |
| To speed up success and shorten duration of diarrhea, concurrently take a probiotic supplement containing strains known to “put a hurtin’ on” C. Difficile. Take probiotic at least 2 hrs away from antibiotics. These include: Saccharomyces boulardi (Florastor); Lactobacillus acidophilus and Bifidobacterium spp. (Dr. Mercola Complete probiotics); Lactobacillus rhamnosus GG (LGG) (Culturelle). It is advisable to take a quality, multi-strain probiotic after the standard therapy and continue for at least 6 weeks to restore normal GI tract flora. E.g. Dr. Mercola® Complete Probiotics Also, include natural food probiotics and prebiotics in your diet. | Minimum 50 billion CFU /day (multi-strain/high production quality) X 42 days |
| Some therapy Choices for recurrent Clostridium difficile infection | |
|---|---|
| (From germination of intestinal spores that “escaped” standard therapy or reinfection) | |
Oral vancomycin therapy | |
| Tapering Vancomycin (shown to be effective) | 125 mg 4 times/day X 7 days;125 mg twice daily X 7 days;125 mg once daily X 7 days;125 mg every other day X 7 days125 mg every third day X 14 days |
| Vancomycin PLUS | 125-250 mg 4 times/day X 14 days |
| Rifampin | 150-300 mg twice/day X 14 days |
| or Bacitracin | 25,000 U4 times/day X 14 days |
| Oral Anion-binding substances (binds C. difficile toxins) | |
| Anion-binding resin: Cholestyramine (LoCHOLEST, Prevalite, Questran) slows fecal transit time but also binds C. difficile toxins (Cholestyramine alternative: Eat a banana or banana flakes twice a day) PLUS | 4 g 3-4 times/day X 14 days (but avoid constipation) Must take medications 3 hours apart because the resin of cholestyramine can bind vancomycin |
| Vancomycin | 125-250 mg 4 times/day X 14 days |
| Bentonite clay or Activated charcoal PLUS | See links for dosages / Avoid constipation |
| Vancomycin | 125-250 mg 4 times/day X 14 days |
| Oral probiotic therapy | |
| Saccharomyces boulardii PLUS | 500 mg twice daily for 4 weeks |
| Vancomycin (Vancocin, Vancoled) Reduced relapse rate by 50% in randomized placebo-controlled trial – well tolerated. | 125 mg 4 times/day for 10-14 days |
| Vancomycin (Vancocin, Vancoled) Then after Vancomycin course: Lactobacillus GG (Culturelle, Lactinex) | 125 mg 4 times/day for 10-14 days100 billion organisms 4 times/day X 7-14 days |
| Continued Probiotic Therapy | |
| It is advisable to follow any of the above therapies by taking a quality probiotic supplement for a month or two to restore normal GI tract flora. E.g. Dr. Mercola® Complete Probiotics | Minimum 50 billion CFU /day (multi-strain/high production quality) x 30-60 days |
Joyce AM, Burns DL. Recurrent Clostridium difficile colitis: tackling a tenacious nosocomial infection. POSTGRADUATE MEDICINE / VOL 112 / NO 5 / NOVEMBER 2002










