For those seeking in-depth details on CES
The following is a Chapter Reprint from:
PAIN MANAGEMENT: A PRACTICAL GUIDE FOR CLINICIANS
Daniel L. Kirsch, Ph.D., D.A.A.P.M.
The Textbook of the AmericanAcademyof Pain Management
CRC Press, Boca Raton, Florida, 2001 Revision.
Chapter © copyright 2001 by D. L. Kirsch, Mineral Wells, Texas.
All Rights Reserved
AN INTRODUCTION TO CRANIAL ELECTROTHERAPY STIMULATION
Cranial electrotherapy stimulation (CES) is the application of low-level, pulsed electrical currents (usually not exceeding one milliampere), applied to the head for medical and/or psychological purposes. It is primarily used to treat both state (situational) and trait (chronic) anxiety, depression, insomnia, stress related and drug addiction disorders, but it is also proving indispensable for treating pain patients (Lichtbroun, Raicer & Smith, 2001; Kirsch & Smith, 2000; Thuile & Kirsch, 2000).
Drs. Leduc and Rouxeau of France were first to experiment with low intensity electrical stimulation of the brain in 1902. Initially, this method was called electrosleep as it was thought to be able to induce sleep. Since then, it has been referred to by many other names, the most popular being transcranial electrotherapy (TCET) and neuroelectric therapy (NET). Research on using what is now referred to as cranial electrotherapy stimulation (CES) began in the Soviet Unionduring the 1950’s.
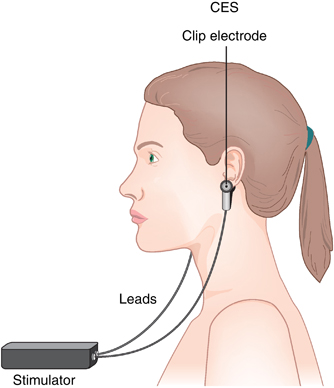
Cranial electrotherapy stimulation is a simple treatment that can easily be administered at any time. The current is applied by easy-to-use clip electrodes that attach on the ear lobes, or by stethoscope-type electrodes placed behind the ears. In the 1960’s and early 1970’s, electrodes were placed directly on the eyes because it was thought that the low level of current used in CES could not otherwise penetrate the cranium. This electrode placement was abandoned over 20 years ago. Recent research has shown that from 1 mA of current, about 5 µA/cm2 of CES reaches the thalamic area at a radius of 13.30 mm which is sufficient to affect the manufacture and release of neurotransmitters (Ferdjallah, 1996).
Anxiety reduction is usually experienced during a treatment, but may be seen hours later, or as late as one day after treatment. Although in some people it may require a series of five to ten daily treatments to be effective. Severe depression often takes up to three weeks to establish a therapeutic effect.
Cranial electrotherapy stimulation leaves the user alert while inducing a relaxed state. Psychologists call this an alpha state. The effect differs from pharmaceutical treatment in that people usually report feeling that their bodies are more relaxed, while their minds are more alert. Most people experience a feeling that their bodies are lighter, while thinking is clearer and more creative. A mild tingling sensation at the electrode sites may also be experienced during treatment. The current should never be raised to a level that is uncomfortable. One 20-minute session is often all that is needed to effectively control anxiety for at least a day, and the effects are usually cumulative. If the patient can only tolerate a small amount of current (<200 µA), due to vertigo or nausea, more time is required. Cranial electrotherapy stimulation may also be used as an adjunct to anxiolytic or anti-depressive medication, but the dosage of medication should then be reduced by approximately one-third. It is also proven to be an effective complimentary treatment along with psychotherapy, biofeedback training, and surgical anesthesia (Kirsch, 1999). For people who have difficulty falling asleep, CES should be used in the morning to avoid the possibility of increased alertness that may interfere with sleep.
Most people can resume normal activities immediately after treatment. Some people may experience an euphoric feeling, or a state of deep relaxation that may temporarily impair their mental and/or physical abilities for the performance of potentially hazardous tasks, such as operating a motor vehicle or heavy machinery, for up to several hours after treatment.
At present, there are over 100 research studies on CES in humans and 20 experimental animal studies (Kirsch, 1999). No significant lasting side effects have ever been reported. Occasional self-limiting headache (1 out of 450), discomfort or skin irritation under the electrodes (1 out of 811), or lightheadedness may occur. A rare patient with a history of vertigo may experience dizziness for hours or days after treatment.
Most cranial electrotherapy stimulators are limited to 600 µA. To put this into perspective, it takes one-half of an ampere to light an ordinary 60 watt light bulb. To truly compare the work done per second by these two different currents, we must multiply the currents by the respective voltages that drive them. The product of current x voltage is a measure of the rate of generation of energy, and is referred to as the power output. By definition, when a device outputs one ampere of current with a one volt driving force, the power output of the device is one watt. Therefore a device producing a maximum output of 600 µA is limited to about 11,000 times less power than the light bulb: (600/1,000,000)amperes x 9 volts = 0.0054 watts. Some people do not even feel this amount of current.
As in many areas of biology and therapy, the evidence of CES effectiveness is empirical. It is generally believed that the effects are primarily mediated through a direct action on the brain at the limbic system, the hypothalamus and/or reticular activating system (Brotman, 1989; Gibson & O’Hair, 1987; Madden & Kirsch, 1987). The primary role of the reticular activating system is the regulation of electrocortical activity. These are primitive brain stem structures. The functions of these areas and their influence on our emotional states were mapped using electrical stimulation. Electrical stimulation of the periaqueductal gray matter has been shown to activate descending inhibitory pathways from the medial brainstem to the dorsal horn of the spinal cord, in a manner similar to ß-endorphins (Salar, 1981; Pert, 1981; Ng, 1975). Cortical inhibition is a factor in the Melzack-Wall Gate Control theory (Melzack, 1975). Toriyama (1975) suggested it is possible that CES may produce its effects through parasympathetic autonomic nervous system dominance via stimulation of the vagus nerve (CN X). Taylor(1991) added other cranial nerves such as the trigeminal (CN V), facial (CN VII), and glossopharyngeal (CN IX). Fields (1975) showed that electrocortical activity produced by stimulation of the trigeminal nerve is implicated in the function of the limbic region of the midbrain affecting emotions. Substance P and enkephalin have been found in the trigeminal nucleus, and are postulated to be involved in limbic emotional brain structures (Hokfelt, 1977). The auditory-vertigo nerve (CN VIII) must also be effected by CES, accounting for the dizziness one experiences when the current is too high. Ideally, CES electrodes are placed on the ear lobes because that is a convenient way to direct current through the midbrain and brain stem structures.
From studies of CES in monkeys, Jarzembski (1970) measured 42% to 46% of the current entering the brain, with the highest concentration in the limbic region. Rat studies by Krupisky (1991) showed as much as a threefold increase in ß-endorphin concentration after just one CES treatment. Pozos (1971) conducted mongrel dog research that suggests CES releases dopamine in the basal ganglia, and that the overall physiological effects appear to be anticholinergic and catecholamine-like in action. Richter (1972) found the size, location, and distribution of synaptic vesicles were all within normal limits after a series of ten, one-hour treatments in Rhesus monkeys. Several studies in stump-tailed macaques and humans revealed a temporary reduction in gastric hypersecretion (Reigel, 1970; Reigel, 1971; Wilson, 1970; Kotter, 1975).
A recent review by Kirsch (1999) of 106 human studies involving 5,439 subjects (4,058 receiving cranial electrotherapy stimulation, while the remainder served as sham-treated or placebo controls) revealed significant changes associated with anxiolytic relaxation responses, such as lowered reading on electromyograms (Gibson, 1987; Forster, 1963; Heffernan, 1995; Overcash, 1989; Voris, 1995), slowing on electroencephalograms (Braverman, 1990; Cox, 1975; Heffernan, 1996; Heffernan, 1997; Krupitsky, 1991; McKenzie, 1971; Singh, 1971), increased peripheral temperature, an indicator of vasodilatation (Brotman, 1989; Heffernan, 1995), reductions in gastric acid output (Kotter, 1975), and in blood pressure, pulse, respiration, and heart rate (Heffernan, 1995; Taylor, 1991).
The efficacy of CES has also been clinically confirmed through the use of 27 different psychometric tests. The significance of CES research for treating anxiety has been reconfirmed through meta-analyses conducted at the Universityof Tulsaby O’Connor (1991), and by Klawansky (1995) at the Department of Health Policy and Management, Harvard School of Public Health.
Seventeen studies conducted follow-up investigations from one week to two years after treatment (Brotman, 1989; Brovar, 1984; Cartwright, 1975; Flemenbaum, 1974; Forster, 1963; Hearst, 1974; Heffernan, 1995; Hochman, 1988; Koegler, 1971; Magora, 1967; Matteson, 1986; Moore, 1975; Overcash, 1999; Patterson, 1988; Smith, 1999; Turaeva, 1967; Weiss, 1973). Sixteen of 16 (100%) reported that at least some of the subjects had a continued improvement after a single CES treatment, or a series of CES treatments. The other follow-up report only commented on safety (Forster, 1963). None of the 17 studies revealed any long term harmful effects.
When restricted to anxiety populations or studies that measured for physiological and/or psychological changes in anxiety, there are 40 scientific studies of CES, involving 1,835 patients. Thirty-four of the 40 (85%) studies reported efficacious results in the treatment of anxiety. Five of the studies on CES (all using the Alpha-Stim) support the effectiveness for managing anxiety during or after a single treatment (Gibson, 1987; Heffernan, 1995; Smith, 1999; Voris, 1995; Winick, 1999).
None of the 6 of 40 (15%) anxiety studies categorized by the authors as having negative or indeterminate results were recent, five were done in the 1970’s, and one in 1980. Three showed both actual treatment and sham groups to improve significantly, most likely because both groups were also taking medications (Levitt, 1975; Passini, 1976; Von Richtofen, 1980). One was a depression study in which the author noted that acute anxiety was not relieved and again, the study did not control for medications (Hearst, 1974). One reported no significant change on anxiety or depression scales, but subjective insomnia improved (P<.05) during active treatment (Moore, 1975). Only one study conducted on a population of insomniacs, with an average duration of symptoms for almost 20 years, did not show any significant change at all in any parameters (Frankel, 1973). [Perhaps the device used in Frankel’s study was defective.]
Cranial electrotherapy stimulation has been well researched and clearly proven to be the most effective, and safest method of treatment for anxiety, and anxiety-related disorders. It is also highly effective for depression and insomnia, muscle tension, fibromyalgia and headaches.As an increasing number of patients seek alternatives to the side effects and potential addiction to mood-altering pharmaceuticals and controlled substances, CES offers a viable solution. It is easy enough to offer CES in a psychologist’s, dentist’s or physician’s office, clinic, or hospital, and chronically stressed patients will find it cost-effective over time to own their own CES device.
Indications
In addition to the primary claims for anxiety, depression insomnia, and pain, CES has been researched with significant results for many other conditions. Smith and Shiromoto (1992) showed it to be highly effective in blocking fear perception in phobic patients. Favorable results have also been reported for labor, epilepsy, hypertension, surgery, spinal cord injuries, chronic pain, arthritis, cerebral atherosclerosis, eczema, dental pain, asthma, ischemic heart disease, stroke, motion sickness, digestive disorders as well as various addictive disorders including cocaine, marijuana, heroin and alcohol abuse(Wharton, McCoy, & Cofer, 1982; Schmitt, Capo, et al., 1984; Smith, 1975; Smith, 1982; Patterson, 1983; Daulouede, 1980; Gomez & Mikhail, 1978; Brovar, 1984; Feighner, Brown, & Olivier, 1973; Overcash & Siebenthall, 1989).
Reflex sympathetic dystrophy (RSD) and fibromyalgia syndrome (FS) are two significant pain diagnoses from primary central and autonomic nervous system etiologies that respond best to CES (Alpher & Kirsch, 1998; Lichtbroun et al., 1999). Adding somatic treatment with MET to these two conditions does not seem to improve the outcomes.
Besides specific pathological disorders, there are a growing number of studies being conducted that show increases in cognitive functions. Michael Hutchison (1986) discussed several mind enhancement techniques in his book Megabrain, devoting chapter 9 to CES as a tool for attaining higher levels of consciousness. Sparked by Hutchison, Madden and Kirsch (1987) completed a study that demonstrated CES to be a useful tool for improving psychomotor abilities. Smith (1999) demonstrated that CES significantly improved stress related cognitive dysfunction, such as attentiondeficit disorder (ADD), after only three weeks of treatment, and maintained the effect through an 18-month follow-up assessment.
Methodology
Cranial electrotherapy stimulation devices are generally similar in size and appearance to TENS units, but produce very different waveforms. Standard milliampere-current TENS devices must never be applied transcranially. CES electrodes can be placed bitemporally, forehead to posterior neck, bilaterally in the hollow just anterior to the mastoid processes, or through electrodes clipped to the earlobes. The ear clip method, developed by the author, is the easiest and possibly most effective electrode placement.
The electrodes must first be wet with an appropriate conducting solution. When using ear clip electrodes, apply them to the superior aspect of the ear lobes, as close to the jaw as possible. Start with a low current and gradually increase it. If the current is too high the patient may experience a painful stinging sensation at the electrodes, dizziness, or nausea. If any of these three symptoms arise, immediately reduce the current and the symptoms will subside in a few moments. After a minute or two, try increasing the current again, but keep it at a comfortable level. It is okay for the patient to feel the current as long as it is not uncomfortable.
The ideal treatment time is 20 to 60 minutes, but some patients may achieve the full benefits of a CES treatment within 10 minutes. Many dentists use it instead of nitrous oxide gas to help relax patients during dental procedures (Winick, 1999). Sometimes these dental procedures last for hours with the patient undergoing CES treatment the entire time.
Although CES treatment is indicated for insomnia, because of the increased alertness some patients find it difficult to fall asleep immediately after a treatment. Accordingly, it is recommended that CES be used at least three hours before going to bed. Also, in most cases after daily treatments for the first week or two, treating every other day is usually more effective than daily treatment.
The CES Experience
During the treatment, most patients will experience a subjective change in their body weight. They may feel heavier at first and then lighter, or they may feel lighter initially. The patient may feel worse during the heavy cycle and this feeling can last for hours or even days in rare cases unless extra treatment time is given. Therefore it is important to continue the treatment if the patient feels heavier at the end of the allotted time, even if it has already been 20 minutes or more. Continue for at least two to five minutes after the patient feels lighter. Not all patients will be aware of these weight-perception changes.
Following CES, most people feel better, less distressed, and more focused on mental tasks. They generally sleep better and report improved concentration, increased learning abilities, enhanced recall, and a heightened state of well-being
Psychologists first described these general feelings during the 1970’s as an alpha state of consciousness. Meditation, biofeedback training, relaxation instructions, chanting, hypnotherapy, and certain religious rituals also produce such states. This is not the same as the alpha brain wave frequency of 8 to 13 Hz. Often, practitioners are confused by device representatives who claim that their particular device will output and entrain a brain to the alpha frequency. There is no evidence to support that CES devices work on an entrainment principle.
Contraindications
There have not been any significant lasting harmful side effects reported in any of the research literature from either MET or CES. As with all electrical devices, caution is advised during pregnancy, and with patients using an older model (pre-1998) demand-type pacemaker.In addition, it is recommended that patients do not operate complex machinery or drive automobiles during and shortly after a CES treatment.
Summary
Microcurrent electrical therapy and cranial electrotherapy stimulation are electromedical modalities that use low level currents that usually do not exceed one milliampere. Beneficial effects have been reported for a wide variety of pain, psychological distress, and addiction-related disorders.
Pain is a complex process encompassing the entire nervous system. To achieve optimal results through electromedical intervention, the peripheral and central nervous systems should both be treated. Cranial electrotherapy stimulation induces a relaxed, alert state. It is a primary modality effective for controlling anxiety, depression, insomnia and generalized stress ubiquitous in pain patients. In addition, there is mounting evidence that CES can enhance cognitive functions. Because of its safety and effectiveness, the combination of MET and CES used with the protocols described here are highly recommended for a broad range of pain and stress-related disorders.
References
1. Lichtbroun AS, Raicer MS, & Smith RB. The use of Alpha-Stim cranial electrotherapy stimulation in the treatment of fibromyalgia. Presented at the 15th annual International Symposium on Acupuncture and Electro-Therapeutics, Columbia University, New York City, October 21-24, 1999.
2. Kirsch DL & Smith RB. The use of cranial electrotherapy stimulation in the management of chronic pain: A review. NeuroRehabilitation. 2000 14:85-94.
3. Thuile C & Kirsch DL. Schmerzen linden ohne chemie: CES, die revolution in der schmerztherapie. IGEM, Austria (in German), 2000.
4. Ferdjallah, Mohammed, Bostick Jr., Francis X. Jr. & Barr, Ronald E. Potential and current density distributions of cranial electrotherapy stimulation (CES) in a four-concentric-spheres model. IEEE Transactions on Biomedical Engineering. 1996. 43(9):939-943.
5. Kirsch DL. The Science Behind Cranial Electrotherapy Stimulation. Medical Scope Publishing, Edmonton, Alberta, Canada. 1999.
6. Brotman P. Low-intensity transcranial electrostimulation improves the efficacy of thermal biofeedback and quieting reflex training in the treatment of classical migraine headache. American Journal of Electromedicine. 1989. 6(5):120-123.
7. Gibson TH & O’Hair DE. Cranial application of low level transcranial electrotherapy vs. relaxation instruction in anxious patients. American Journal of Electromedicine. 1987. 4(1):18-21. Also doctoral dissertation, California School of Professional Psychology, 1983.
8. Madden RE & Kirsch DL. Low intensity transcranial electrostimulation improves human learning of a psychomotor task. American Journal of Electromedicine. 1987. 2(2/3):41-45.
9. Salar G, Job I. et al. Effect of transcutaneous electrotherapy on CSF b-endorphin content in patients without pain problems. Pain. 1981. 10:169-172.
10. Pert A, Dionne R, Ng LKY& et al. Alterations in rat central nervous system endorphins following transauricular electroacupuncture. Brain Research. 1981. 224:83-94.
11. Ng LKY, Douthitt T. & et al. Modification of morphine-withdrawal syndrome in rats following transauricular electrostimulation: an experimental paradigm for auricular electroacupuncture. Biological Psychiatry. 1975. 10:575-580.
12. Melzack R. Prolonged pain relief by brief, intense transcutaneous somatic stimulation. Pain. 1975. 1:373-375.
13. Toriyama M. Ear acupuncture anesthesia. Ear Throat. 1975. 47:497-501.
14. Taylor DN. Effects of cranial transcutaneous electrical nerve stimulation in normal subjects at rest and during stress. Doctoral dissertation, Brooklyn College of the City University of New York, 1991. Pages 1-96.
15. Fields WR, Tacke RB & Savana BS. Pulpal anodal blockade of trigeminal field potentials elicited by tooth stimulation in the cat. Experimental Neurology. 1975. 47:229-239.
16. Hokfelt T, Ljungdahl A & et al. Immunohistological analysis of peptide pathways possibly related to pain and analgesia: enkephalin and substance P. Proceedings of the National Academy of Science. 1977. 74:3081-3085.
17. Jarzembski WB, Sanford JL & Sances A, Jr. Evaluation of specific cerebral impedance and cerebral current density. Annals of the New York Academy of Sciences. 1970. 170:476-490.
18. Krupitsky EM, Burakov GB, Karandashova JaS & et al. The administration of transcranial electric treatment for affective disturbances therapy in alcoholic patients. Drug and Alcohol Dependence. 1991. 27:1-6.
19. Pozos RS, Richardson AW & Kaplan HM. Electroanesthesia: A proposed physiologic mechanism. In Reynolds, D.V., & Anita Sjoberg (Eds.) Neuroelectric Research. Springfield, Charles Thomas, 1971. Pages 110-113.
20. Richter WR, Zouhar RL, Tatsuno J & et al. Electron microscopy of the macaca mulatta brain after repeated applications of electric current. Anesthesiology. 1972. 36(4):374-377.
21. Reigel DH, Dallmann DE, Christman NT & et al. Physiological effects of electrotherapeutic currents in the primate and man. In Wageneder FM & St. Schuy (Eds.), Electrotherapeutic Sleep and Electroanesthesia. Vol. II, Amsterdam, Excerpta Medica, 1970. Pages 158-165.
22. Reigel DH, Larson SJ, Sances A, Jr. & et al. Effects of electrosleep currents on gastric physiology. In Reynolds, D.V. & Sjoberg, Anita (Eds.) Neuroelectric Research. Springfield, Charles Thomas. 1971. 24:226-229.
23. Wilson AS, Reigel D, Unger GF & et al. Gastric secretion before and after electrotherapeutic sleep in executive monkeys. In Wageneder, FM, & St. Schuy (Eds.), Electrotherapeutic Sleep and Electroanesthesia. Vol. II, Amsterdam, Excerpta Medica, 1970. Pages 198-206.
24. Kotter GS, Henschel EO, Hogan Walter J. & et al. Inhibition of gastric acid secretion in man by the transcranial application of low intensity pulsed current. Gastroenterology. 1975. 69:359-363.
25. Forster S, Post BS & Benton JG. Preliminary observations on electrosleep. Archives of Physical and Medical Rehabilitation. 1963. 44:81-89.
26. Heffernan M. The effect of a single cranial electrotherapy stimulation on multiple stress measures. The Townsend Letter for Doctors and Patients. 1995. 147:60-64, October.
27. Overcash SJ & Siebenthall A. The effects of cranial electrotherapy stimulation and multisensory cognitive therapy on the personality and anxiety levels of substance abuse patients. American Journal of Electromedicine. 1989. 6(2):105-111.
28. Voris MD. An investigation of the effectiveness of cranial electrotherapy stimulation in the treatment of anxiety disorders among outpatient psychiatric patients, impulse control parolees and pedophiles, Delos Mind/Body Institute, Dallas, Texas, 1995. Pages 1-19.
29. Braverman E, Smith R, Smayda R & Blum K. Modification of P300 amplitude and other electrophysiological parameters of drug abuse by cranial electrical stimulation. Current Therapeutic Research. 1990. 48(4):586-596.
30. Cox A & Heath RG. Neurotone therapy: A preliminary report of its effect on electrical activity of forebrain structures. Diseases of the Nervous System. 1975. 36:245-247.
31. Heffernan M. Comparative effects of microcurrent stimulation on EEG spectrum and correlation dimension. Integrative Physiological and Behavioral Science. 1996. 31(3):202-209.
32. Heffernan M. The effect of variable microcurrents on EEG spectrum and pain control. Canadian Journal of Clinical Medicine. 1997. 4(10):4-11.
33. Krupisky EM, Katznelson YaS, Lebedev VP & et al. Transcranial electrostimulation (TES) of brain opioid structures (BOS): experimental treatment of alcohol withdrawal syndrome (AWS) and clinical application. Presented at the Society for Neuroscience Annual Meeting, New Orleans, November 10-15, 1991.
34. McKenzie RE, Rosenthal SH & Driessner JS. Some psychophysiologic effects of electrical transcranial stimulation (electrosleep). American Psychiatric Association, Scientific Proceedings Summary. 1971. Also in The Nervous System and Electric Currents, Wulfsohn, N.L., and Sances, A. (Eds.) Plenum: New York, 1976. Pages 163-167.
35. Singh B, Chhina GS, Anand BK & et al. Sleep and consciousness mechanism with special reference to electrosleep. Armed Forces Medical Journal (New Delhi), 1971. 27(3):292-297.
36. O’Connor ME, Bianco F & Nicholson R. Meta-analysis of cranial electrostimulation in relation to the primary and secondary symptoms of substance withdrawal. Presented at the 12th annual meeting of the Bioelectromagnetics Society, June 14, 1991.
37. Klawansky S, Yeung A, Berkey C, Shah N & et al. Meta-analysis of randomized controlled trials of cranial electrotherapy stimulation: efficacy in treating selected psychological and physiological conditions. Journal of Nervous and Mental Diseases. 1995. 183(7):478-485.
38. Brovar A. Cocaine detoxification with cranial electrotherapy stimulation (CES): A preliminary appraisal. International Electromedicine Institute Newsletter. 1984. 1(4).
39. Cartwright RD & Weiss MF. The effects of electrosleep on insomnia revisited. Journal of Nervous and Mental Disease. 1975. 164(2):134.
40. Flemenbaum A. Cerebral Electrotherapy (Electrosleep): An open clinical study with a six month follow-up. Psychosomatics. 1974. 15:20-24.
41. Hearst ED, Cloninger R, Crews EL & Cadoret RJ. Electrosleep therapy: A double-blind trial. Archives of General Psychiatry. 1974. 30:463-66.
42. Hochman R. Neurotransmitter modulation (TENS) for control of dental operative pain. Journal of the American Dental Association. 1988. 116:208-212.
43. Koegler RR, Hick SM & Barger J. Medical and psychiatric use of electrosleep (transcerebral electrotherapy). Diseases of the Nervous System. 1971. 32(2):100-104.
44. Magora F, Beller A, Assael MI & Askenazi A. Some aspects of electrical sleep and its therapeutic value. In Wageneder, F.M. and St. Schuy (Eds). Electrotherapeutic Sleep and Electroanaesthesia. Excerpta Medica Foundation, International Congress Series No. 136. Amsterdam, 1967. Pages 129-135.
45. Matteson MT & Ivancevich JM. An exploratory investigation of CES as an employee stress management technique. Journal of Health and Human Resource Administration. 1986. 9:93-109.
46. Moore JA, Mellor CS, Standage KF & Strong H. A double-blind study of electrosleep for anxiety and insomnia. Biological Psychiatry. 1975. 10(l):59-63.
47. Overcash SJ. A retrospective study to determine the effect of cranial electrotherapy stimulation (CES) on patients suffering from anxiety disorders. American Journal of Electromedicine. 1999. 16(1):49-51.
48. Patterson M, Firth J & Gardiner R. Treatment of drug, alcohol and nicotine addiction by neuroelectric therapy: Analysis of results over 7 years. Journal of Bioelectricity. 1984. 3(1&2):193-221.
49. Smith RB. Cranial electrotherapy stimulation in the treatment of stress related cognitive dysfunction with an eighteen month follow-up. Journal of Cognitive Rehabilitation. 1999. 17(6):14-18.
50. Turaeva VA. Treatment of eczema and neurodermatitis by electrosleep. In Wageneder, FM & St. Schuy (Eds). Electrotherapeutic Sleep and Electroanaesthesia. International Congress Series No. 136. Excerpta Medica Foundation, Amsterdam. 1967. Pages 203-204.
51. Weiss MF. The treatment of insomnia through use of electrosleep: an EEG study. Journal of Nervous and Mental Disease. 1973. 157(2):108-120.
52. Smith RB & Shiromoto FN. The use of cranial electrotherapy stimulation to block fear perception in phobic patients. Current Therapeutic Research. 1992. 51(2):249-253.
53. Wharton GW, et al. The use of cranial electrotherapy stimulation in spinal cord injury patients. A poster study presented at the American Spinal Injury Association Meeting, New York, and at the Texas ASIA meeting in Houston, 1982, 1983.
54. Schmitt R, Capo T, Frazier H. & Boren D. Cranial electrotherapy stimulation treatment of cognitive brain dysfunction in chemical dependence. Journal of Clinical Psychiatry. 1984. 45:60.
55. Smith RB. Electrosleep in the management of alcoholism. Biological Psychiatry. 1975. 10:675.
56. Smith RB. Confirming evidence of an effective treatment for brain dysfunction in alcoholic patients. Journal of Nervous and Mental Disorders. 1982. 170(5):275-278.
57. Patterson M. Getting Off the Hook. Wheaton, Illinois: Harold Shaw Publishers, 1983.
58. Daulouede J. Une nouvelle methode de sevrage des toxicomanes par utilisation du courant de Limoge (A new method of eliminating drug addiction using Limoge’s current). Annales Medic-Psychologiques. 1980. 138(3):359-370.
59. Gomez E & Mikhail AR. Treatment of methadone withdrawal with cerebral electrotherapy (electrosleep). British Journal of Psychiatry. 1978. 134:111-113.
60. Feighner JP, Brown SL & Olivier JE. Electrosleep therapy: A controlled double-blind study. Journal of Nervous and Mental Disorders. 1973. 157:121.
61. Alpher EJ & Kirsch DL. Traumatic Brain Injury and full body reflex sympathetic dystrophy patient treated with cranial electrotherapy stimulation. American Journal of Pain Management. 1998. 8(4):124-128.
62. Hutchison M. Megabrain. New York: Beech Tree Books, William Morrow.
63. Winick RL. Cranial electrotherapy stimulation (CES): a safe and effective low cost means of anxiety control in dental practice. General Dentistry. 1999. 47(1):50-55.