Plantar Fasciitis - Pain under the heel
Overview
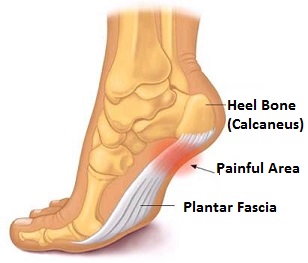
Plantar Fasciitis (aka. plantar heel pain syndrome, heel spur syndrome, runner’s heel or painful heel syndrome) is a degenerative, commonly inflammatory condition of the plantar fascia felt as discomfort / pain under the heel of the foot.
As the foot flattens, the plantar fascia stretches and begins to pull away from the heel causing pain
- The plantar fascia is a non-elastic ligament, comprised of thick fibrous connective tissue (fascia) extending from heel to toes. It creates the arch of the foot and has an important role in the mechanical function of the foot affecting gait
- Collagen is the main component of the plantar fascia. The PF contains closely packed bundles of collagen fibers forming a wavy pattern parallel to the direction of pull having great tensile strength.
- Pain is consequential to an abnormality or injury to the plantar fascia. Causing traction beyond its stretching ability, usually where it is attached to and pulls away from the heel bone (calcaneus). The other end of the plantar fascia splays and attaches to the metatarsal bones at the ball of the foot
Tension in the plantar fasciitis is critical to maintaining foot arch and serves as a shock absorber for foot and leg
Symptoms of plantar fasciitis
- Dull, intermittent pain. May progress to a sharp, but sustained knife-like pain
- Pain is typically worse immediately after getting out of bed, after sitting, when climbing stairs or after intense activity. Usually eases off throughout the day, but returns after intense or increased physical activity or prolonged weight-bearing
- Pain can be sufficient to cause sufferer to limp with heel lifted off the ground. In the long-term, this can worsen the problem by affecting gait
The mechanics of walkingAfter the heel makes contact with the ground, the tibia turns inward and the foot pronates (rolls inward), stretching the plantar fascia and flattening the arch to accommodate irregularities in the walking surface. |
With aggravating factors, repetitive movements (E.g. walking / running) cause multiple micro-tears in the plantar fascia, weakening the foot arch. This further increases strain on the plantar fascia
Plantar fasciitis typically occurs only in one foot
Plantar fasciitis can dramatically affect physical mobility and also lead to heel spurs. Microscopic tearing of plantar fascia can cause inflammation of the heel bone (calcaneus) leading to the production of bone growths (spurs), which may or may not be painful
Plantar fasciitis is the most common cause of heel pain
- An estimated 10% of U.S. population will experience plantar heel pain in their lifetime Crawford F et al, 2000
- Accounts for 11-15 % of all foot symptoms. Pfeffer G et al, 1999
- 2 million people in the U.S. are treated for plantar fasciitis on an annual basis
Possible causes /aggravating factors of plantar fasciitis
Causes are not well understood and probably multi-factorial
Higher risk of occurrence in those:
- With high arch or flat feet
- Who are male (especially those aged 40-70 who are active) – possibly due to greater weight /speed/impact
- Wearing badly fitting footwear – especially with insufficient arch support
- With rigidity in feet
- Having an improper gait / poor biomechanics
- Running / dancing on their toes – E.g. ballerinas, dancers, long-distance or downhill runners
- Regularly running on hard, irregular, or soft (Eg. sand) surfaces
- Who have gained weight or who are obese
- With occupations requiring prolonged weight-bearing
- With leg-length discrepancy
- With weakened / atrophied muscles – The elderly, those with peripheral motor neuropathy (E.g. a possible symptom of diabetes)
Athletic injury of the foot typically from running or sports involving intensive overuse of the feet without sufficient acclimating build-up. Usually occurs over time resulting from repetitive trauma, possibly from running on hard, soft or irregular surfaces, steep inclines; especially affects those having a high arch
Turning sole inward or outward
Treatment options for plantar fasciitis
PF is considered a self-limited condition – since >80% of cases resolve / heal within 12 months regardless of therapy
“An ounce of prevention . . .”
Best treatment is prevention. This involves being sensitive to early warning signs and using preventative exercises; after a hiatus, runners should warm up gradually to a full workout program
Prefer conservative therapies to surgery
General recommendations
- Cease activities known to induce trauma / inflammatory stress on plantar fascia. Athletes will need to be patient to allow time to heal
- Speedy treatment prevents further problems developing as a result of an altered gait in response to foot pain. Such problems may affect the knee, hip and/or spine and will need to be addressed to facilitate complete healing.
- Plantar Fascia strengthening / Stretching Exercises. With the overall goal of stretching the tightened plantar fascia along the foot arch. There is a growing study / experience-supported opinion that a program of non-weight-bearing stretching exercises specific to the plantar fascia is superior to the standard program of weight-bearing Achilles tendon-stretching exercises
Exercises to stretch tightened plantar fascia
- Other stretching / strengthening exercises may be necessary to strengthen weak muscles affecting the problem. E.g. strengthening calf muscles
- Prevent sheets at the foot of the bed from putting too much pressure on the feet
- Wear good arch-supportive footwear and a well-cushioned heel
- Night splinting to hold ankle joint in a neutral position. Prevents foot from becoming flexed in the night
Nutritional therapy
Connective tissue repair / regeneration
- Vitamin C
- Antioxidant property fights inflammation
- Increase PF tensile strength – essential for building procollagen (collagen precursor).
- Recommended Dose: 1 – 2 g ascorbic acid /day
- Zinc. Generally recognized for its positive effect on the immune system
- Works with C to increase PF tensile strength. Zinc insufficiency (common in high stress people or those with injuries) implicated in delayed wound healing
- Recommended Dose: 15 mg zinc / day
- Glucosamine – foundational substrate for several compounds associated with repair and regeneration of connective tissue, including hyaluronic acid and other glycosaminoglycans (GAGs)
- Recommended Dose: 500mg glucosamine sulfate 3 x /day
Anti-inflammatories
- Vitamin C
- Bromelain – family of proteolytic enzymescommonly used for treating soft tissue injuries and treating inflammation
- Reduces swelling / pain;
- Increases fibrinolysis (promotesplasminogen à plasmin). Taussig SJ and Batkin S, 1988.
- Recommended Dose: 500 -2000 mg/day (with enzymatic activity of at least 2,000 mcu/g)
- Omega-3 EPA and DHA. Notable anti-inflammatory fatty acids
Also see general recommendations to counter and control chronic inflammation:
Inflammation – Can’t live with it, Can’t live without it!
NIR Class 4 laser therapy
NIR class 4 laser therapy restores the flow of nutrients and oxygen to inflamed tissue and increases cellular waste removal. This allows the cells to repair themselves more quickly than when left untreated
One particular study is sometimes referenced to denounce the efficacy of laser treatment for plantar fasciitis. However, it is noted that this study used a very low power (30mW) laser, which would not penetrate tissue like the higher-powered lasers used in NIR class 4 laser therapy. Basford JR et al, 1998
Other healing alternatives to surgery include
(without reference to their efficacy):
- Injections / Medication. For temporary relief E.g. anti-inflammatories such as steroidal corticosteroid injections and NSAIDS E.g. celecoxib, ibuprofen, naproxen
- Extra-corporeal shock wave therapy (ESWT). Pulses of high-pressure sound waves
- Orthotics / Heel cups / Arch support
- Magnetic insoles
- Ultrasound
- Strapping/Taping
- Therapeutic ultrasound
- Chiropractic (manipulative therapy)
- Soft tissue therapy / massage
- Heat
- Ice. Anti-inflammatory effect
- Acupuncture
Stuber et al reviewed the efficacy of randomized, controlled, clinical trials (published in English between1980 and 2005) involving different conservative modalities to treat plantar fasciitis. Kent Stuber and Kevyn Kristmanson, 2006
Plantar Fasciitis (PF) Strengthening and stretching exercises
The following exercises are designed to stretch the tightened plantar fascia along the foot arch
Plantar fascia rolling
- Slowly move the foot arch back and forth over a tin can or tennis ball
- Ice the Foot Arch by rolling a frozen plastic water bottle or juice container under the foot for only ~5 minutes (overexposure to ice may inflict tissue damage).

Plantar fascia stretching
The following study concluded that:“A program of non-weight-bearing stretching exercises specific to the plantar fascia is superior to the standard program of weight-bearing Achilles tendon-stretching exercises for the treatment of symptoms of proximal plantar fasciitis.” BACKGROUND: Approximately 10% of patients with plantar fasciitis have development of persistent and often disabling symptoms. A poor response to treatment may be due, in part, to inappropriate and nonspecific stretching techniques. We hypothesized that patients with chronic plantar fasciitis who are managed with the structure-specific plantar fascia-stretching program for eight weeks have a better functional outcome than do patients managed with a standard Achilles tendon-stretching protocol. METHODS: One hundred and one patients who had chronic proximal plantar fasciitis for a duration of at least ten monthswere randomized into one of two treatment groups. The mean age was forty-six years. All patients received prefabricated soft insoles and a three-week course of celecoxib, and they also viewed an educational video on plantar fasciitis. The patients received instructions for either a plantar fascia tissue-stretching program (Group A) or an Achilles tendon-stretching program (Group B).All patients completed the pain subscale of the Foot Function Index and a subject-relevant outcome survey that incorporated generic and condition-specific outcome measures related to pain, function, and satisfaction with treatment outcome. The patients were reevaluated after eight weeks. RESULTS: Eighty-two patients returned for follow-up evaluation. With the exception of the duration of symptoms (p < 0.01), covariates for baseline measures revealed no significant differences between the groups. The pain subscale scores of the Foot Function Index showed significantly better results for the patients managed with the plantar fascia-stretching program with respect to item 1 (worst pain; p = 0.02) and item 2 (first steps in the morning; p = 0.006). Analysis of the response rates to the outcome measures also revealed significant differences with respect to pain, activity limitations, and patient satisfaction, with greater improvement seen in the group managed with the plantar fascia-stretching program. CONCLUSIONS: A program of non-weight-bearing stretching exercises specific to the plantar fascia is superior to the standard program of weight-bearing Achilles tendon-stretching exercises for the treatment of symptoms of proximal plantar fasciitis. These findings provide an alternative option to the present standard of care in the nonoperative treatment of patients with chronic, disabling plantar heel pain. BF Digiovanni, et al. 2006 In contrast, the “stair stretches” are standard weight-bearing stretching exercises designed to stretch the calf muscles and Achilles tendon. |
Instructions for plantar fascia stretching

Photo: Jonathan Cluett, M.D.
- Hold the ends of the towel (or sheet or rubber Thera-Band) and loop the middle around your toes.
- Keep the knee straight and toes pointing up.
- Pull the towel ends, pulling the toes towards body until a stretch is felt in the fascia.
Above study recommends doing ten reps, holding stretch for 10 seconds three times a day. Doing the FIRST set BEFORE getting out of bed in the morning
Lorem ipsum dolor sit amet, consectetur adipiscing elit. Ut elit tellus, luctus nec ullamcorper mattis, pulvinar dapibus leo.
References
Basford JR, Malanga GA, Krause DA, Harmsen WS. A randomized controlled evaluation of low-intensity laser therapy: plantar fasciitis. Arch Phys Med Rehabil.1998 Mar;79(3):249-54. PubMed
BF Digiovanni, et al. “Plantar Fascia-Specific Stretching Exercise Improves Outcomes in Patients with Chronic Plantar Fasciitis. A Prospective Clinical Trial with Two-Year Follow-Up” J. Bone Joint Surg. Am., Aug 2006; 88: 1775 – 1781.Link
Crawford F, Atkins D, Edwards J. Interventions for treating plantar heel pain. Cochrane Database Syst Rev 2000;(3):CD000416. Update in: Cochrane Database Syst Rev 2003;(3):CD000416.
Kent Stuber, BSc, DC,Kevyn Kristmanson, BSc, DC.Conservative therapy fpr plantar fasciitis: a narrative review of randomized controlled trials J. Can Chiropr Assoc.2006 June;50(2): 118-133. PubMed
Pfeffer G, Bacchetti P, Deland J, et al. Comparison of custom and prefabricated orthoses in the initial treatment of proximal plantar fasciitis. Foot Ankle Int 1999;20:214-221.
Taussig SJ, Batkin S. Bromelain, the enzyme complex of pineapple (Ananas comosus) and its clinical application. An update. J Ethnopharmacol 1988;22:191-203.