
Type 2 diabetes (T2D)


What is T2D?
T2D is an inflammatory disease stemming from having too many sugar molecules in the blood
Damaging compounds called advanced glycation end products (AGEs), are produced when simple sugars, such as glucose or fructose molecules, bind by a non-enzymatic process (called glycosylation), with proteins, lipids and nucleic acids. AGEs alter the structure and function of various cells and tissues throughout the body and can promote damage to blood vessels, peripheral nerves and organ tissues with an associated inflammatory reaction. E.g. AGEs derived from glucose binding to hemoglobin (oxygen-carrying protein in red blood cells) are shown to accelerate atherosclerosis (buildup of arterial plaque), contributing to an increase in the risk of a heart attack or stroke.
Chronic (ongoing) inflammation causes damage to body’s cells / tissues. Such damage can lead to health problems, including heart attacks, stroke, kidney disease or infections. Donath & Shoelson, 2011 In patients with chronic diabetes, AGEs are also implicated in peripheral arterial disease (which can cause gangrene and lead to amputations), peripheral neuropathy (nerve damage in the limbs), retinopathy (eye damage), and nephropathy (kidney damage). An example study is that high-circulating AGEs and RAGE predict cardiovascular disease mortality among older community-dwelling women. Semba RD, Ferrucci L, Sun K, et al. Advanced glycation end products and their circulating receptors predict cardiovascular disease mortality in older community-dwelling women. Aging Clin Exp Res. 2009;21(2):182-190. doi:10.1007/BF03325227
AGEs can also enter the body from exogenous sources such as diet (especially foods exposed to high temperatures, during e.g. grilling, frying, or toasting) or tobacco smoke.
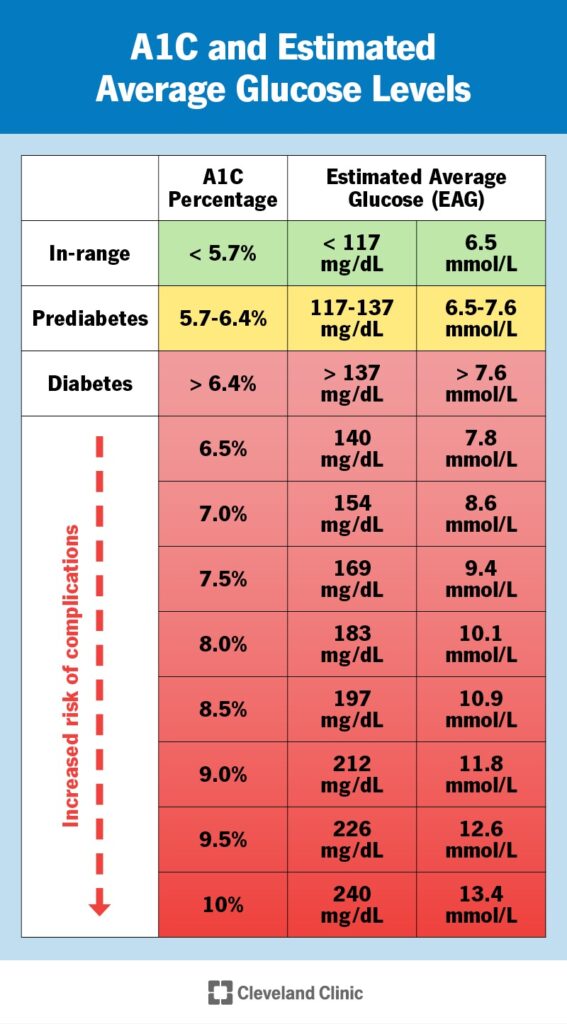
Suspected T2D is measured with an A1C test. Measures the average amount of glucose in the blood over the past few months – reported as a percentage. Result is used to detect prediabetes, T2D and monitor control of type 1 diabetes. More specifically, the A1c test measures the average amount of glucose attached to hemoglobin (part of the red blood cell (RBC) that carries oxygen). This glucose stays attached for about 3 months (about the life of the RBC) and so gives a better picture than a singular blood sugar test.
What is causing T2D?
(1) Too many carbs
The current T2D epidemic occurring in the Western world is mainly a consequence of the overconsumption of carbohydrates i.e. sugar and starches, which metabolize to the simple sugars: glucose, galactose and fructose in the small intestine and are then transported into the bloodstream. When blood glucose concentration exceeds a certain level, in order to prevent health problems, the pancreatic beta cells produce insulin to remove glucose from the blood (storing it as energy). Over time, when a person chronically overconsumes carbohydrates, cells eventually become resistant to insulin’s “message” to take in glucose from the blood – a situation termed insulin Resistance (IR). SInce the blood glucose is still present, the pancreas ups insulin output in a futile effort to solve the high sugar problem, but the cells are just not responding as they used to.
(2) An overzealous immune reaction due to an imbalance of Omega-6 and omega-3 fats
Another contributing factor in T2D involves the overzealous inflammatory response to tissue-damage (resulting from excessive carb consumption), as a consequence of the underconsumption of anti-inflammation-promoting fatty acids.
An imbalance of anti-inflammatory (Primarily Omega-3 fats) and inflammatory (Omega-6 fats) exacerbates Insulin Resistance. Tessaro et al, 2014
In addition to telling liver and muscle cells to store glucose as glycogen, another effect of elevated insulin is to upregulate production of certain enzymes (delta-5, delta-6 and delta-9 desaturases (abbreviated d5d, d6d and d9d) responsible for converting essential fatty acids sitting in cell membranes from one form to another.
- D5d. Converts DGLA into the omega-6 fatty acid AA, being the most potent source of inflammatory eicosanoids (Series 2 Prostaglandins, Series 2 thromboxanes, Series 4 leukotrienes).
D6d. Converts omega-6 linoleic acid (LA) to the omega-6 DGLA fatty acid, which is the most potent source of anti-inflammatory eicosanoids (Series 1 Prostaglandins and Series 1 Thromboxanes. Unfortunately, d6d production declines with age, whereas d5d does not, giving an edge to the d5d conversion of DGLA to inflammatory AA, particularly in the over 50’s.
Thus, people promoting high insulin levels by eating a lot of carbohydrates together with an inadequate intake of anti-inflammatory omega-3 fats (thereby creating a shortage of anti-inflammatory eicosanoids in their cell membranes) put their body into a chronic low-level pro-inflammatory state (with its long-term negative health consequences) by creating an excess of inflammatory eicosanoids over anti-inflammatory eicosanoids. In a healthy body, inflammatory fatty acid AA has a balanced presence with anti-inflammatory fatty acids: EFA and DGLA in cell membranes to yield an appropriately balanced immune response to damaged tissue. https://www.gdx.net/core/interpretive-guides / Essential-Metabolic-Fatty-Acids-Interp-Guide.pdf In a positive feedback cycle, any inflammation promotes more insulin resistance, leading to further increases in blood sugar and insulin levels — and more inflammation. The fix for IR is to inhibit delta 5 desaturase production and AA production and enhance d6d production and DGLA production. To prevent great tissue damage, eicosanoids also control the inflammatory resolution and tissue repair process. Imbalances in eicosanoid synthesis have been reported to drive chronic inflammation, which deregulates signaling pathways and/or cellular events leading to abnormal immune functions. In particular, circulating and local mediators, such as eicosanoids, interleukin- (IL-) 1β, tumor necrosis factor- (TNF-) α, IL-6, IL-8, macrophage migration inhibitory factor (MIF), and free radicals, create a state of low-chronic inflammation in diabetic patients. Inflammation may lead to diabetes progression, including damage to the kidneys (diabetic nephropathy), eyes (diabetic retinopathy), nerves (diabetic neuropathy), and cardiovascular system. Fernando et al, 2014
(3) Obesity / Fat cells
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2246086/
(4) Insulin Resistance (IR)
Chicken and egg situation. In a study published in the August online version of Diabetes, H. Henry Dong and his colleagues at the University of Pittsburgh showed that a protein called FOXO1 serves as a master switch that turns on the expression of another key inflammatory cytokine, interleukin 1-beta, which also interferes with insulin signaling. Normally insulin keeps FOXO1 in check; it “rapidly inhibits FOXO1” by moving it out of the nucleus so it can be targeted for degradation, Dong says. But when a person becomes insulin-resistant and pancreatic cells no longer produce enough insulin to overcome the resistance, activity of FOXO1 increases. Also https://europepmc.org/article/med/28213398#free-full-text
Alternative treatments for type 2 diabetes (T2D)
Berberine shown to be as effective as diabetes medication for T2D
The potential glucose-lowering effect of berberine was noted when it was used for diarrhea in diabetic patients. This yellow herb also lowers blood pressure, fights parasites, and more
Berberine is a powerful plant extract, which can effectively lower blood sugar. Its benefits in addition to most diabetic medications are that it can also help with weight loss and improve heart health, is effective against diarrhea, is anti-inflammatory and antimicrobial, killing intestinal parasites, Candida albicans, and possibly Methicillin-resistant staph aureus. Lan J et al, 2015
Berberine actions are : Pang B et al, 2015
- Decrease insulin resistance, making the blood sugar lowering hormone insulin more effective.
- Increase glycolysis, the breakdown of glucose inside cells.
- Decrease glucose production in the liver.
- Slow the digestion of carbohydrates.
- Increase the number of beneficial bacteria in the gut.
Berberine is a bioactive plant extract that comes from several different types of plants: including goldthread, Oregon grape root, barberry, tree turmeric and goldenseal. It has been used in both Ayruvedic and Chinese medicine for over 2500 years..
Several impressive studies show that berberine can lower blood glucose as effectively as the drug metformin – without the negative side effects! One peer-reviewed study published in the journal Metabolism compared berberine in one group to metformin (Glucophage) in another group. The berberine group had very similar blood sugar-lowering effects as the metformin group. Another peer-reviewed study in Journal of Clinical Endocrinology found that berberine had a similar glycemic-lowering effect to Metformin. Both studies found that berberine also effectively reduced the patients’ A1c, triglycerides, LDL cholesterol, and blood pressure – three things that metformin cannot do. These are the results from the Metabolism study:
- Hemoglobin A1c decreased from 9.5% to 7.5% (about a 21% reduction)
- Fasting blood glucose (FBG) decreased from 190.8 to 124.2 mg/dl
- Postprandial blood glucose (PBG) decreased from 356.4 to 199.8 mg/dl
- Triglycerides from 100.5 to 79.2 mg/dl
Berberine works by stimulating uptake of glucose into the cells, improves insulin sensitivity, and reducing glucose production in the liver. This review published in the International Journal of Endocrinology further expanded on berberine’s role in treating type diabetes: “BBR [berberine] is used to treat diabetic nephropathy (DPN), diabetic neuropathy (DN), and diabetic cardiomyopathy due to its antioxidant and anti-inflammatory activities.”
How does berberine work?
Berberine works by activating a metabolism-regulating enzyme within the body’s cells – called AMPK (adenosine monophosphate activated protein kinase). AMPK regulates a variety of biological activities that normalize lipid, glucose, and energy imbalances – something you want working for you. Metabolic syndrome, a precursor to diabetes, occurs when these AMPK pathways are switched off., which triggers high blood sugar, high cholesterol, high triglycerides and energy issues. AMPK shifts energy to cellular repair and maintenance. Activating AMPK produces similar benefits for diabetes and metabolic syndrome as do exercise, dieting and weight loss.
Berberine and weight Loss
Easy average weight loss of 5 pounds. When overweight adults took 500mg of berberine 3 times daily for 12 weeks. The researchers note that, “…berberine has potential clinical application in reducing visceral fat and controlling obesity.” Hu Y et al, 2012.
Berberine has the ability to inhibit fat storage and also improves insulin function, leptin and adiponectin. Leptin is a very powerful hormone produced by fat cells. It tells your brain whether you should eat or not. Leptin is the way your fat cells speak to your brain. If Leptin signaling is working, when fat stores are full, they cause a surge in leptin which tells your brain to stop eating and storing fat. The problem is of course, when this signaling goes awry, it causes excessive eating and fat storage.
Adonipectin is a hormone secreted by fat cells that helps control glucose regulation and fatty acid oxidation. Obese people are often low in adonipectin, but berberine helps to increase adonipectin which helps to normalize metabolic function.
So, the bottom line here is that berberine could reduce the size of your fat cellsand cut down on the number of them as well.
Berberine is also thought to enhance brown fat, which is a heat-generating special type of fat that burns energy instead of storing it. It is loaded with active mitochondria cells that convert this fat into energy which produces heat. This animal study shows how berberine increases energy expenditure, helps burn fat, improves cold tolerance and enhances active brown adipose tissue.
Berberine for Memory and Cognitive Function
Blood sugar levels, insulin sensitivity and diabetes go hand in hand with memory and cognitive dysfunction. In fact, it is now thought that high blood sugar and diabetes are connected to an increased risk of Alzheimer’sdisease. Berberine has been found to enhance memory function in some animal studies, by preserving a brain chemical, acetylcholine, that is important for memory, focus and cognition. The result for berberine was improved learning and memory, along with lower oxidative stress.
How to take berberine
Take 500-600 mg berberine two to three times a day 20-30 minutes before a meal. Most studies found 500 mg to be a safe dose, and it is probably a good idea to build up slowly, starting at one dose / day. Take berberine 20-30 minutes before a meal with 8-12 ounces of water to avoid any stomach upset and to take advantage of the post meal glucose and lipid spike that occurs. Look for a berberine product with a standardized berberine extract so that the dosages and strength are consistent.
When taking berberine supplement, insulin may need to be cut back significantly, so blood sugar must be frequently monitored. The ideal situation is that you will eventually be able to stop other pharmaceutical diabetes medications.
Berberine side effects
Pregnant and nursing women should not take berberine.
If you have a medical condition or are on any medications, including antibiotics: it is recommended that your physician monitor your blood sugar and current medication levels. Diabetics who are using diabetic medications should use caution when using berberine to avoid dangerously low blood sugar levels. People with low blood pressure should also be careful, since it can naturally lower blood pressure.
Primary side effects of this natural extract are minor: possible cramping, diarrhea, flatulence, constipation or mild stomach pain. Use smaller dosages after meals to avoid most of these side effects.
In addition to its huge benefits for diabetes, berberine is helpful for other health issues, including:
- Anti-aging
- Gastrointestinal infections
- Heart disease
- High cholesterol
- Hypertension (high blood pressure)
- Immune challenges
- Joint problems
- Low bone density
References
Donath MY, Shoelson SE. (2011) Type 2 diabetes as an inflammatory disease. Nat Rev Immunol. ;11(2):98-107. PubMed
Fernando HG Tessaro, Thais S. Ayala, Joilson O. Martins (2014) Lipid Mediators Are Critical in Resolving Inflammation: A Review of the Emerging Roles of Eicosanoids in Diabetes Mellitus; BioMed Research International Volume 2015, Article ID 568408 pdf
Semba RD, Ferrucci L, Sun K, et al. (2009) Advanced glycation end products and their circulating receptors predict cardiovascular disease mortality in older community-dwelling women. Aging Clin Exp Res.;21(2):182-190. PubMed
Omega-6 oils http://www.cureddiabetes.com/insulin-resistance.html
Article by Cat Ebeling, co-author of the best-seller: The Diabetes Fix
Lan J, Zhao Y, Dong F, Yan Z, Zheng W, Fan J, Sun G. Meta-analysis of the effect and safety of berberine in the treatment of type 2 diabetes mellitus, hyperlipemia and hypertension. J Ethnopharmacol. 2015 Feb 23;161:69-81. doi: 10.1016/j.jep.2014.09.049. Epub 2014 Dec 10. PMID: 25498346.
Kittelsrud J, Ronan PJ, Munger K, Downey T, Bohlen K, Callahan L, Munson V, Jahnke M, Marshall LL, Nelson K, Huizenga P, Hansen R, Soundy TJ, Davies GE. Lipid-lowering effect of berberine in human subjects and rats. Phytomedicine. 2012 Jul 15;19(10):861-doi: 10.1016/j.phymed.2012.05.009. Epub 2012 Jun 26.PMID:22739410
Pang B, Zhao LH, Zhou Q, Zhao TY, Wang H, Gu CJ, Tong XL. Application of berberine on treating type 2 diabetes mellitus. Int J Endocrinol. 2015;2015:905749. doi: 10.1155/2015/905749. Epub 2015 Mar 11. PMID: 25861268; PMCID: PMC4377488.
.










