What is a goiter?
A goiter is an enlarged thyroid gland. A normal gland weighing ~1/2 oz can increase up to ~2 pounds. The whole gland can enlarge (called diffuse goiter) or there can be one or more small nodules. Enlargement is not due to physical inflammation, but is a thick tissue growth caused by the presence of chronic or agressive thyroid stimulating hormone (TSH); this may occur for a variety of reasons, including, for example, iodine deficiency, pregnancy, inflammatory thyroid damage or having diagnosed (or undiagnosed) Hashimoto’s thyroiditis.
Most nodules (lumps) are cysts filled with fluid, called cystic nodules); nodules can also contain the stored form of thyroid hormones, collectively called colloid; solid nodules have minimal fluid or colloid.
A goiter can be associated with:
- Hyperthroidism / An overactive thyroid / Excessive thyroid hormones
- Hypothroidism /An underactive thyroid / Insufficient thyroid hormones
- Normal thyroid hormone levels
Physical characteristics of a goiter can be:
- Symmetrical or Nodules or enlargement are in just one part of the gland
- Diffuse (spread out, generalized, smooth, as in Grave’s disease) or solitary (if only a small area is enlarged; commonly benign cysts, nodules)
- Nodules are benign or malignant (cells in nodule have the ability to spread outside the thyroid gland)
Non-toxic, toxic or endemic goiter?
Non-toxic Goiter
- Diffuse (spread out) or Nodular (i.e. lumps; 1 = solitary thyroid nodule / more than 1 = multinodular goiter)
- Thyroid hormone production is normal
- Non-cancerous
- Not associated with Hyperthroidism, Hypothyroidism, or inflammation
Toxic DIFFUSE or NODULAR Goiter
- Diffuse Toxic Goiter (a.k.a. Graves Disease or exophthalmic goiter) (involves autoimmune-antibodies / auto-antibodies) / Toxic Nodular Goiter (is not an autoimmune disease);
- Excessive secretion of thyroid hormones;
- Causes signs and symptoms of hyperthyroidism;
Endemic Goiter (Goitrous hypOthyroidism)
- Inability to make sufficient thyroid hormone
- Associated with Hypothroidism
- Most common cause is Hashimoto’s thyroiditis
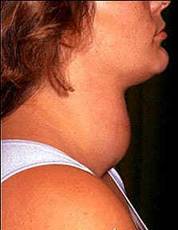
Symptoms
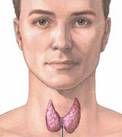
A goiter is seen as a swelling at the front base of the neck
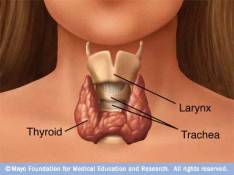
The enlarged thryroid compresses the trachea (windpipe) and esophagus. This can lead to such symptoms as:
- Coughing;
- Waking up with the feeling of being unable to breathe;
- Sensation of food stuck in upper throat
Causes
A goiter could occur as a result of:
- Inadequate iodide levels. This being the most common cause of goiter worldwide, particularly prevalent in areas of iodine-deficient soil; referred to as ENDEMIC goiter.
- Hashimoto’s Thyroiditis. An autoimmune thyroiditis; anti-thyroid antibodies attack thyroid causing damage/inflammation leading to hypothyroidism
Ord’s thyroiditis. Seen particularly in Europe; an atrophic form of autoimmune thyroiditis;
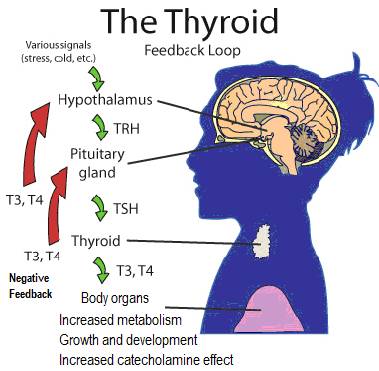
- Increase in thyroid stimulating hormone (TSH). This is in response to a problem with usual/normal thyroid hormone production;
- Malfunctioning/damaged/ inflamed thyroid. Damage possibly results from insufficient iodine intake;
- Excessive presence of goitrogens. These can block thyroid access to iodine needed for TH production and create unused thyroglobulin (Tg);
- Hypothyroidism. Since low hormone levels stimulate TH production;
- Some drugs. Lithium inhibits release of TH; amiodarone may induce inflammatory damage to thyroid;
- Thyroid Cancers / Benign tumors (nodules). May cause a multinodular goiter (solid or fluid-filled lumps, called nodules);
- Pregnancy. The pregnancy hormone human chorionic gonadotropin (HCG) may cause slight thyroid enlargement;
- Graves Disease / Diffuse Toxic goiter. Autoimmune disease stimulates thyroid to be overactive;
- Too much iodine ???; Currently researching this.
Risk Factors
Anyone from birth onwards can have goiters. Some common risk factors are:
- A lack of iodine
- Being female / Pregnancy / Menopause
- Age > 40
- Family history of autoimmune disease
- Radiation exposure. Medical radiation to neck/chest area or general exposure from nuclear sources
- Certain medications. The heart drug amiodarone (e.g. Pacerone, Cordarone), lithium (e.g. Lithobid)
References
Marine D, Kimball BS. (1917) The prevention of simple goiter in man. J Lab Clin Med; 3:40-48.
Marine D. (1923) Prevention and treatment of simple goiter. Atl Med J; 26:437-442.