
Stomach ulcers (a.k.a. gastric ulcers) - A sore on your stomach lining
What is a stomach (gastric ulcer)?
A stomach ulcer is a sore in the stomach lining caused by irritation over a period of time. Something weakens and breaks the protective lining of the stomach allowing stomach acid to act on the wound. Usually due to stress, the stomach cannot produce enough mucus to protect the stomach lining, resulting in the soft tissue below the lining becoming exposed, thus allowing gastric juices (strong stomach acid and pepsin enzymes) to come into direct contact with the wound. This irritates the soft tissue causing gastritis (inflammation of the stomach lining), until eventually, the constant irritation causes a sore, called an ulcer. The body tries hard to repair the damage, replacing epithelial cells every 2-3 days.
A stomach ulcer is a type of PEPTIC ulcer. Peptic ulcers can occur in the stomach (gastric ulcer), lower esophagus (esophageal ulcers), or the upper small intestine i.e. duodenum (duodenal ulcers). About 80-90% of peptic ulcers are in the duodenum (since the stomach mucosal glands have usually produced and emptied out too much acid chyme to be neutralized by the pancreatic juices). The next most common ulcers are in the stomach.
Interesting tidbit: Pig stomach ulcers occur at the top of the stomach and human ulcers toward the bottom.
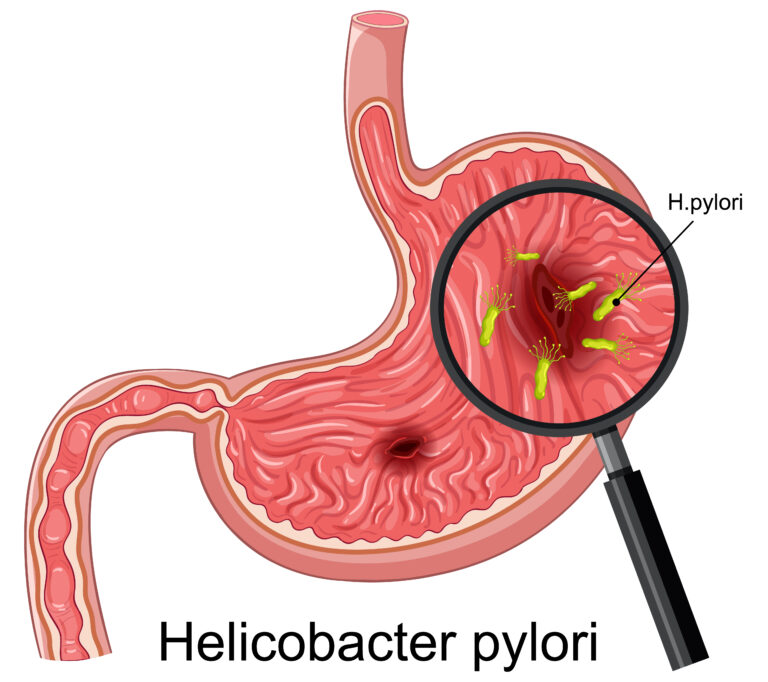
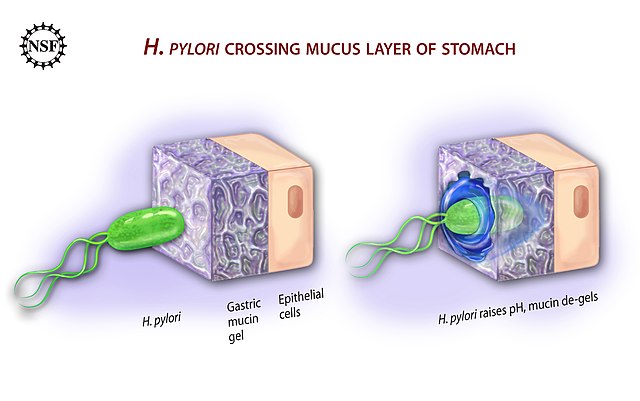
The most common cause of tissue damage in peptic ulcers is the Helicobacter Pylori (H. Pylori) bacteria. Previously known as Campylobacter pylori, this gram-negative, helically-shaped microaerophile can colonize in the gastric epithelium. After establishing its residence, it weakens the protective mucous coating of the stomach (and also intestinal duodenum), thus allowing stomach acid access to the sensitive lining beneath. Both the acid and the bacteria irritate the lining and cause a sore, or ulcer.
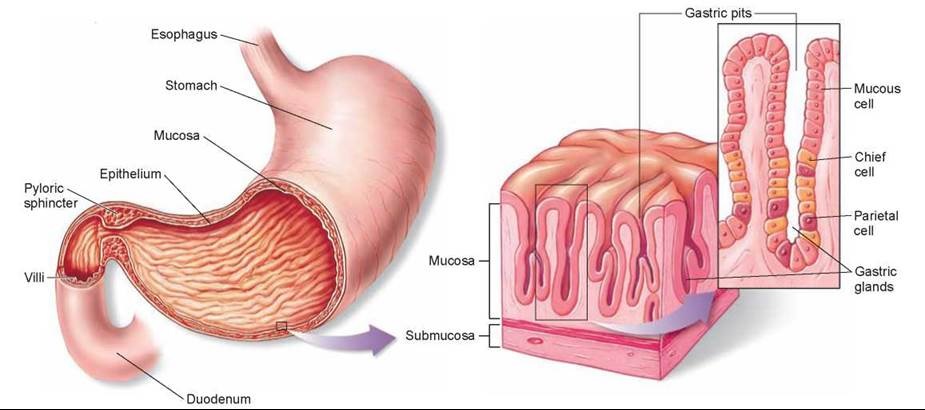
Some relevant stomach anatomy 101 |
|---|
The stomach lining (gastric mucosa / mucus membrane)This 1 mm thick, velvety smooth, protective mucus membrane lines the stomach. It contains mucus secreting glands and columnar epithelial cells. Stomach lining integrity and repair. TGF-alpha produced by gastric epithelial cells stimulate epithelial cell proliferation. TGF-alpha also enhances mucus secretion and inhibits stomach acid production. Other cytokines such as fibroblast growth factor and hepatocyte growth factor have been shown to enhance healing of gastrointestinal ulcers in experimental models. |
Gastric / Stomach acid
Predominately composed of hydrochloric acid (HCl). Also water, electrolytes (sodium, potassium, calcium, phosphate, sulfate, and bicarbonate), and other organic substances, such as mucus, enzymes (pepsins), and protein. Has a pH of about 1.5 – 3.5
Primary purpose is for partial digestion of proteins in the stomach. Unravels proteins and activates digestive pepsin enzymes to break down (hydrolize) the long chains of amino acids in food proteins (peptides) into shorter polypeptide chains and so make their complete digestion easier in the small intestine. Sufficient HCl keeps the pepsin enzyme working at its best.
Of interest, some absorption of water, alcohol and weakly acidic drugs occurs in the stomach. E.g. Aspirin is a weakly acidic drug, and being mostly un-ionised in the acid stomach, is more easily absorbed by the stomach mucosal cells via diffusion. However, overall, most absorption takes place in the small intestine. ~20% of water and alcohol is absorbed from the stomach.
Gastric gland parietal and chief cells
Parietal cells
Parietal cells produce hydrochloric Acid (HCl), bicarbonate (HCO3-), intrinsic factor (needed for red blood cell maturation and B12 absorption) and most of the water in gastric juice. HCl production is controlled by the hormone GASTRIN to produce HCl only when pH goes above ~1.5, and slows due to negative feedback around a pH of 2. GASTRIN increases in response to gastric distention (via vagus nerve) and insufficent acidity when food enters stomach. Parietal cells produce an average 1.35 liters of HCl / day to create a stomach acid average pH of ~2.5 (i.e. ~250,000 times more acidic than blood). Parietal cells secrete hydrogen ions to be combined with chlorine ions to form HCl, which drains into the bottom of the gland and passes into the stomach by ATP-powered magnesium-dependent proton pumps (H+/K- ATPase). HISTAMINE and ACETYLCHOLINE also control HCl production
Parietal cells produce bicarbonate ions (HCO3-) in exchange for chlorine ions (Cl-) used for HCl production. After eating, bicarbonate is secreted into the blood by gastric mucusal cells resulting in a slight elevation of blood pH known as the “alkaline tide”. This process maintains a balanced pH inside the parietal cell.
Prostaglandins (cell-localized, hormone-like substances present in most all tissues / body fluids) and PPIs omeprazole (Losecâ„¢ or Prilosecâ„¢) and lansoprazole (Prevacidâ„¢) inhibit acid secretion by the parietal cells. Prostaglandins are members of the eicosonoid family of lipid molecules. In particular, the prostaglandins PGE2 and PGI2 (prostacyclin) are well recognized cell-protectors. Their other protective modus operandi is that they stimulate mucosal mucus and bicarbonate secretion, increase mucosal blood flow, and limit back diffusion of acid into the stomach lining epithelium. Chief cellsChief cells produce pepsinogen (converted to the pepsin enzyme for digesting protein). Like HCl, production is also controlled by food consumption (via the vagus nerve) and the hormones/neurotransmitters: GASTRIN, HISTAMINE and ACETYLCHOLINE. Gastric mucosa and mucus cells (foveolar cells)Foveolar cells produce mucus to protect the stomach lining (gastric mucosa) from corrosive stomach acid. Located in the neck of the gastric pits, these surface cells cover the entire gastric mucosa to provide a thick mucus layer, which both lubricates the lining to help food masses travel through the stomach more easily and protects against damage. This protective mechanism prevents the lining from being digested by its own protein “breakdown” enzymes, also aided by the parietal cell production of bicarbonate, which is secreted by gastric mucus cells to result in a neutral pH close to the lining. Mucus is a slimy material composed of mainly mucin cells and inorganic salts suspended in water. Abundant carbohydrates on mucin molecules bind to bacteria, which helps to prevent them colonizing in the epithelial lining. Gastric mucosal lining also contains acid-resistant lipoproteins Parietal cell bicarbonate production brings bicarbonate to the surface for secretion by gastric mucous secreting cells. |
What are the symptoms of gastric / stomach ulcers?
Early symptoms (May or may not present)
Pain. The major ulcer symptom is a burning / gnawing feeling in the stomach area lasting from about 30 minutes up to 3 hours.
- Pain is often interpreted as heartburn, indigestion or hunger.
- Pain usually occurs in the upper abdomen. But sometimes it may occur below the breastbone.
- For some, the pain occurs immediately after eating. For others, the pain may not occur until hours after eating.
- Pain frequently awakens the person at night (typically around 2:00 am).
- Weeks of pain may be followed by weeks of not having pain.
- Pain can be relieved by drinking milk, eating, resting, or taking antacids.
Pernicious anemia. In addition to HCl, the stomach’s mucosal gland parietal cells also secrete intrinsic factor, a polypeptide needed for intestinal absorption of vitamin B12. SInce B12 is required for the production of red blood cells, parietal cell damage can reduce intrinsic factor causing a type of anemia (low red blood cell count), called pernicious anemia
Other early symptoms:
- Recurrent vomiting;
- Blood in the stool. Bleeding ulcers can result in significant blood loss requiring hospitalization. Indicators include black stools, light headedness, dizziness
- Scar tissue. Thick tissue can develop after ulcer injury to stomach lining making it harder for food to pass through GI tract. Indicators include vomiting and weight loss.
Advanced symptoms
Any of the following symptoms may potentially indicate serious damage to the stomach lining, which may lead to tissue rupture and thus require hospitalization. Seek urgent attentionif you experience:
- A sudden, sharp, stinging pain in the stomach that will not go away.
- Suddenly vomiting fresh blood, or blood of a dark brown color
- Stools contain blood, or are of a dark brown/black color without explanation. Feeling dizzy or light-headed can be a symptom of internal bleeding from an ulcer. Blood loss can be significant;
- Signs of shock: fainting, excessive sweating, confusion
- Abdomen feels hard to the touch
- Abdominal pain worsens with movement, but eases if you lie still
Possible Consequences of a Stomach Ulcer
- Agitates nerves around ulcer causing great pain
- Can cause hemorrhages from the erosion of a major blood vessel
- Perforation of the stomach lining or small intestine (i.e. a hole) causing an infection. Consequences include peritonitis (inflammation) or obstruction of the GI tract because of spasm or swelling in the area of the ulcer. A sign of a perforated ulcer is sudden, severe abdominal pain.
What are the causes and risk factors of gastric / stomach ulcers?
What causes a stomach ulcer?
H. Pylori
H. pylori is a common bacteria infecting about half of the world’s population, with higher prevalence in developing countries.
The bacteria H. Pylori are responsible for ~75% of all gastric ulcers. In these cases, ulcers are a consequence of their burrowing into the stomach lining and causing inflammatory damage. H. Pylori presence is normally controlled by a sufficient acidity level in the stomach. . H. pylori can survive in the harsh acidic environment of the stomach because they produce the urease enzyme that promotes ammonia production around them to neutralize stomach acid. However, this study found that their glucose metabolism was irreversibly inhibited at the normal healthy stomach acid pH of <3.5.
Nobel Prize recipient Marshall induced gastritis in himself by consuming H. Pylori. He was then able to treat the gastritis using a 14 day dual therapy with bismuth salts and metronidazole. Marshall and Warren went on to show that antibiotics are effective in the treatment of many cases of gastritis. In 1994, the Nation Institutes of Health (USA) published an opinion stating that most recurrent gastric ulcers were caused by H. pylori, and recommended that antibiotics be included in the treatment regimen. Wikipedia
Bacteria usually enter the body via food and drink but may also be contacted through mouth-to-mouth contact such as kissing. Researchers have found H. pylori in the saliva of some infected people.
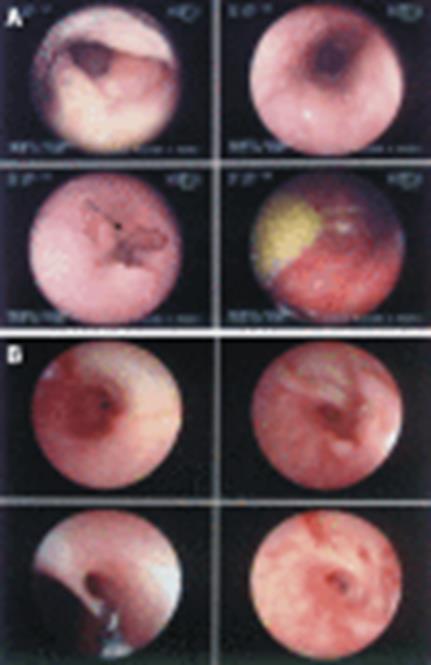
Rapid urease test (RUT) (Also called campylobacter-like organism (CLO) test). Used to diagnose the presence of H. Pylori in a biopsy sample taken from stomach’s gastric mucosa at ulcer site during gastroscopy.
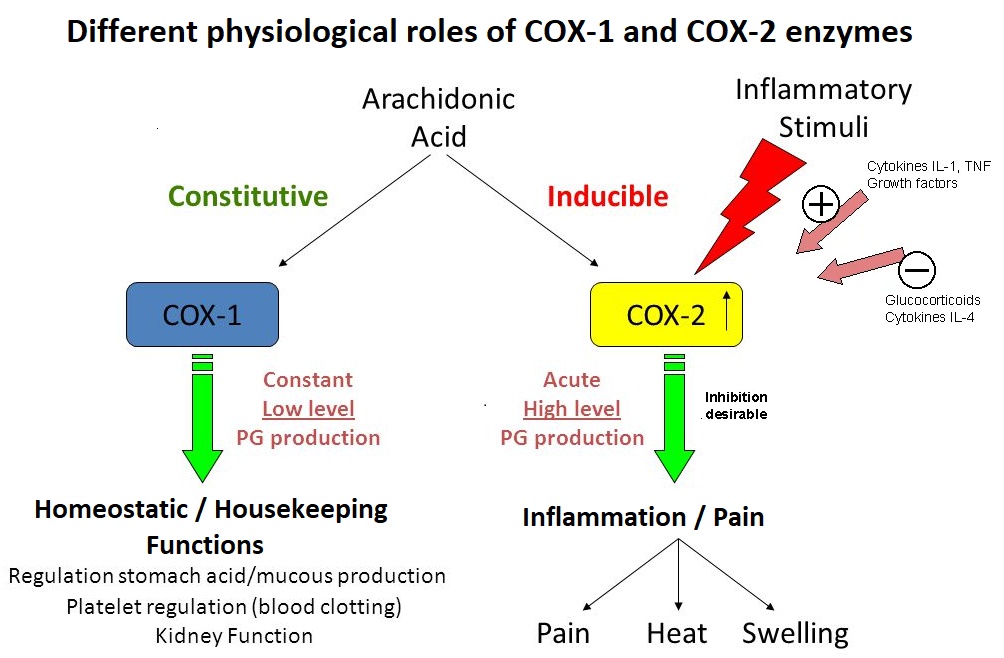
Cox-1 inhibiting NSAIDS (Non-steroidal anti-inflammatory drugs)
Regular, excessive or prolonged use of traditional (COX-2 and COX-1 enzyme inhibiting) NSAIDs is a well recognized cause of peptic ulcers and gastritis (inflammation of the stomach lining). Traditional NSAIDS include aspirin (Beyer®), ibuprofen (Motrin®, Advil®), naproxen (Aleve®) ; The more recent selective COX-2 enzyme inhibitors include Celebrex® and the infamous rafecoxib (Vioxx®, recalled in 2004 after being responsible for an estimated 60,000 deaths due to heart problems). Traditional NSAIDs (Not COX-2 selective) inhibit the COX-1 enzyme in the GI tract, reducing prostanoid synthesis from arichidonic acids (AAs). In particular, reducing prostacyclin (PGI2) and prostaglandin PGE2 with their protective effects for the stomach lining mucosal cells (gastric mucosa) can lead to erosion, ulceration, perforation and hemorrhage.
Prostaglandins prostacyclin (PGI2) and PGE2 are crucial to reducing acid secretion by gastric mucosa’s parietal cells Dini, 2017, and maintaining healthy gastric mucosa by increasing blood flow to damage site and increasing mucus secretion to better protect lining from stomach acid.
COX-1 inhibiting NSAIDs reduce prostaglandins PGI2 (prostacylin), PGD2, PGE2 PGF2α-, and thromboxane TXA2.
Chart of Specific Eicosonoid (including prostaglandins) Effects
Risk increases in women and anyone older than 60. Some NSAIDS are stronger COX-1 inhibitors than others.
Malignant tumor
A malignant tumor causes about 4% of gastric ulcers
Risk factors
Risk factors for developing a stomach ulcer
- Stress
- Excess alcohol consumption. Alcohol has the potential to harm the stomach lining by stimulating gastric juice production (intended to digest protein molecules), even when food is not present.
- Family history of ulcers
- Smoking
- Use of corticosteroids.
- Zollinger-Ellison syndrome
Improper diet, irregular or skipped meals. Dietary factors causing stomach ulcers in pigs (mammals with one stomach, like us) are:
- Low protein / Low fiber diets.
- Levels of wheat in excess of 55%.
- Deficiencies of vitamin E or selenium.
- Diets containing high levels of iron, copper or calcium and/or low in zinc.
- Diets with high levels of POLYUNSATURATED fats.
- Diets based on skimmed milk.
- Chronic disorders such as liver disease, emphysema, rheumatoid arthritis may increase vulnerability to ulcers
Note: Spicy food CANNOT CAUSE stomach ulcers, but can aggravate an existing stomach ulcer.
Risk factors for serious complications, such as stomach lining perforation or bleeding ulcers
- The elderly and women;
- Having rheumatoid arthritis, severe systemic disease or previous history of gastroduodenal bleeding;
- Using anti-thrombotic medication, corticosteroids, or high doses of NSAIDs;
PPIs and antibiotics are the mainstream method of treating stomach ulcers
Standard treatments
TRIPLE and QUADRUPLE therapies. The standard anti-H. pylori treatments use PPIs and antibiotics in TRIPLE therapy (clarithromycin with amoxicillin or metronidazole and a proton pump inhibitor (PPI) or ranitidine bismuth citrate ) or QUADRUPLE therapy (proton pump inhibitor, bismuth, tetracycline, and metronidazole or tinidazole).
Bismuth. Bismuth (a heavy metal) exerts bactericidal effect on H. pylori by different ways, including reducing adherence of the bacteria to the gastric mucosa. Bismuth administered together with metronidazole and clarithromycin, causes resistant H. pylori strains to become more susceptible. Bismuth Therapy in Gastrointestinal Diseases (pdf) . Used alone, bismuth suppresses but does not eradicate H. pylori.
Bismuth also aids healing by protecting against acid and pepsin secretions by covering the lesion and promoting mucosal protective factors such as prostaglandin, epidermal growth factor, and bicarbonate secretion. Available as the active ingredient in Pepto bismol (1 tablet: Bismuth subsalicylate 262 mg; study doses used 120mg 4 times/day, or 240 mg twice/day)
Due to its potential toxicity when used long-term, it is generally recommended that treatment periods with any bismuth-containing compound should last no longer than 6-8 weeks, followed by 8-week bismuth-free intervals.
These standard therapies raise three main objections:
- The increase in the prevalence of H. pylori resistance to antibiotics. In the 90’s, triple therapy resulted in >90% eradication, but by 2010 due to antibiotic resistance, this rate dropped to ~70%. Agudo et al 2010, Agudo et al 2010a, De Francesco et al. 2009.
- Antibiotics destroy your beneficial intestinal flora. Now known to be crucial for health.
- PPIs prevent production of stomach acid. Vital for:
- Protein, vitamin and mineral digestion (especially vitamin B12, calcium, magnesium, copper and zinc). HCl also plays an important role in signaling the pancreas to release digestive enzymes.
- First line of defense against ingested microbes and prevents microbial overgrowth. E.g. bacteria (such as H. pylpori) and fungi (such as candida/yeast).
Proton Pump Inhibitors (PPIs)
PPIs reduce stomach acid production to stop stomach acid irritating ulcer . PPI drugs include antoprazole, lansoprazole, rabeprazole, esomeprazole and omeprazoles.
PPIs have potentially serious adverse side effects:
- Reducing stomach parietal cell HCl acid production reduces protein digestion in the stomach. Obviously, the body needs protein.
- Bacterial overgrowth may develop in the stomach in the absence of acid. Bacterial metabolism of dietary nitrites may then lead to the eogenous production of carcinogenic N-nitroso compounds Kalant, 1998 Vermeer, 2001
- Patients who receive PPIs have a higher incidence of hospital-acquired pneumonia and Clostridium difficile infection. The normal stomach acidity is an important host defense against ingested pathogens Dial, 2004
- In rodents, enterochromaffin-like cell (ECL) tumors and carcinoid tumors have developed using PPIs. Viste, 2004 ECLs reside in the gastric mucosa glands near parietal cells and aid gastric acid production by releasing HISTAMINE.
Alternative treatments for gastric / stomach ulcers
Early recognition is the key to curing a stomach ulcer
By recognizing the symptoms of a stomach ulcer as early as possible, the spread of the ulcer can be arrested and fully cured within a few weeks. Ignoring the symptoms could lead to the spreading of the ulcer, causing a lot of pain and discomfort, plus the possibility of serious damage requiring constant medication.
Treatment goals
Short-term goals
- Eradicate H. pylori (in most stomach ulcer cases, these bacteria have colonized in the epithelium lining the gastric mucosa)
- Protect the ulcer / sore from further irritation.
(a) Reduce secretion / pH of gastric acid
(b) Aid gastroprotection i.e. Counteract damage to ulcer / gastric mucosa by ways unrelated to inhibition of acid secretion i.e. Coat ulcer, promote mucin production by mucus cells, remove irritant factors from diet
- Aid healing / repair of stomach lining
Long term goals (post treatment)
- Restore healthy pH of gastric acid to prevent return of H. pylori. May require a supplement of betaine HCl (hydrochloride) before meals. Promotes production of additional hydrochloric acid in the stomach.
- Avoid causes and lower risk factors of getting a stomach ulcer. Especially use hygienic practices to avoid H. Pylori contamination in food and drink. Wash hands after using the bathroom. H. Pylori is also a major risk factor for stomach cancer.
Omega-3 EPA and Omega-6 GLA fatty acids
Omega-3 EPA (in fish oil) and omega-6 GLA (in blackcurrant, borage and evening primrose oils) provide fatty acids that can be converted to Series 1 and 3 anti-inflammatory eicosanoids, in competition for COX enzymes with omega-6 AA fatty acids (in abundance in today’s typical seed oil rich diet), which convert to generally inflammatory eicosanoids. EPA is found in fish oil. Eicosanoids – Cell’s “First Responders”
Polyphenol treatments for stomach ulcers
Plant polyphenols have several properties that can kill H. Pylori, protect the stomach mucosal lining and heal stomach ulcers. They do this by stimulating and upregulating the body’s own natural antioxidant / anti-inflammatory defense systems.
Polyphenols – Antioxidant / Anti-inflammatory / Anti-cancer effects
A variety of polyphenols have been found to inhibit COX-2 enzyme, O’Leary et al, 2004
Grapefruit seed extract (Citrus paradisi)
Grapefruit seed extract reduces ulcers, kills H.Pylori, and is gastroprotective (i.e. counteracts stomach lining damage)
Grapefruit seeds have been shown to possess antibacterial (including anti-H.Pylori), antiviral and antifungal properties. Such anti-microbial properties are attributed to the antioxidative activity of citrus polyphenol flavonoids found in grapefruit, including naringinin, catechins, epicatechin, epicatechin-3-O-gallate and dimeric, trimeric and tetrameric procyanidins. Heggers, 2002; Reagor, 2002; Proteggente, 2002
Naringenin is a major bioactive flavonoid in grapefruit (responsible for its bitter taste). Naringinin exhibited potent anti-H. pylori activity in vitro Bae et al, 1999 and was implicated in protecting liver cells against injury [Blankson, 2000]. Naringenin was reported to exhibit gastroprotection against gastric injury in rats predominantly due to an increase in mucus secretion, with the suggestion of involvement of endogenous protective prostaglandins (PGs) Motilva, 1994
Study also found that this extract in minute doses causes dose-dependent reduction of acute gastric lesions induced in rats.
GSE heals ulcers in rats. As reported by BBC News, in May 2005, researchers headed up by Dr. Thomas Brzozowski at Jagiellonian University, in Poland, used GSE extract to heal stomach ulcers in rats. Brzozowski et al, 2005;
The study authors concluded that GSE’s beneficial effects were due to:
- Its antibacterial and antioxidant properties
- Significantly increasing blood flow at the ulcer sites;
- Mucosal generation of protective prostaglandin PGE2;
- Preserving body’s antioxidant SOD enzyme activity;
- Reducing gastric acid production (also increased plasma GASTRIN levels, which may be a secondary effect to inhibiting gastric acid production; release of GASTRIN promotes ulcer healing); rats pretreated at 10mg GSE/kg before inducing ulcers had a 50% reduction in gastric acid secretion;
- Reducing free radical-dependent lipid peroxidation.
- Protective effect in the stomach may also involve endogenous prostaglandins (PGs) derived from COX-1 and COX-2 enzyme activity and neuropeptides released from afferent sensory nerves.
Probiotics
Reduce but do not completely eradicate H. Pylori
Manuka Honey (Leptospermum scoparium)
Take a tablespoon of Manuka Honey UMF 10+ or higher (UMF goes up to 20+) before meals 3 times and before bedtime. This honey (made from New Zealand bees feeding on tea tree bushes) has antibacterial, antibiotic, antifungal, anti-inflammatory properties due to its rich polyphenol content Cianciosi, 2018 and can cure most stomach problems such as Barrett’sesophagus, gastritis and stomach ulcers. Reported to eradicate H. Pyrori within a month.
Herbs / Plants
- Panax ginseng. Atsushi et al, 2010
- Turmeric. Shown to very successfully kill H. pylori . Turmeric is also one of the top herbal treatments for cancer.
- Garlic. Sivam, 2001
- Licorice root extract (Glycyrrhiza glabra). In vitro study found that glycyrrhetinic acid inhibited 79.3% (23/29) of H. pylori strains tested at ≤50 mg/L. [Krausse et al, 2004]. Prevents H. Pylori adhesion to gastric mucosa Wittschier, 2009. Orally administered glycyrrhizic acid is almost completely hydrolysed into glycyrrhetinic acid in the stomach and absorbed in the intestinal tract.
- Amaranth seed extract. Its ability to scavenge endogenous ROS was shown to account for the maintenance, integrity and homeostasis of gastric mucosa. Zayachkivsha et al, 2005
- Capsaicin extract. In chili peppers. Reduces gastric lesions
- Other herbal extracts. Several herbs extracted in methanol have been shown to inhibit the growth of H. Pylori in vitro at different minimal inhibitory concentrations (MICs). These herbs, which visibly inhibit growth after overnight incubation, include Myristica fragrans (nutmeg seed), Zingiber officinale (ginger rhizome/root) , Rosmarinus officinalis (rosemary leaf), Achillea millefolium (yarrow), Foeniculum vulgare (fennel seed), Passiflora incarnata (purple passionflower leaf), Origanum majorana (oregano leaf) . Mahady et al, 2005. Achillea millefolium (yarrow) PubMed; Myristica fragans (Nutmeg seed) PubMed All these herbs are available as extracts.
| Studies of effects of substances on stomach ulcers (Note: Most studies were with rats or mice) | ||||
|---|---|---|---|---|
| Substance / Extract | Reduces gastric acid production | Kills H.Pylori | Gastroprotective | Effective Dose |
| Grapefruit seed extract (GSE) | Brzozowski et al, 2005; | Bae et al, 1999 Brzozowski et al, 2005; Heggers, 2002; Reagor, 2002; Proteggente, 2002; | Brzozowski et al, 2005; Blankson, 2000; Motilva, 1994; | |
| Licorice root extract | Krausse et al, 2004; Wittschier, 2009 | Wittschier, 2009 Jalilzadeh-Amin et al, 2015 | ||
| Turmeric | yes | |||
| Garlic | Sivam, 2001 | |||
| Manuka honey | Cianciosi, 2018 | Yes | ||
| Probiotics | Reduce population | |||
| Amaranth seed extract | Zayachkivsha et al, 2005 | |||
| Panax ginseng | Atsushi et al, 2010 | 100mg/kg | ||
Protect / coat stomach mucosa
For bleeding ulcers, consume non-irritating fiber-containing mucilage. The following foods help protect the stomach lining and are easy to digest and nutritious, but be aware that most of these do not have any direct affect on H. Pylori.
- Slippery Elm Bark
- Psyllium seed
- Guar gum
- Flaxseed (consume 2 tsp. fresh-ground flaxseed mixed in milk or plain yogurt a couple times / day).
Licorice root extract (Glycyrrhiza galabra). Used against peptic ulcers as an alternative to bismuth in quadruple therapy.
- G. galabra protects against acid and pepsin secretions by covering the lesion and promoting mucosal protective factors. Asi, 2008
- G. galabra has anti-H. pylori effects. Similar to bismuth.
- G. galabra supports local prostaglandins that promote mucus secretion and cell proliferation in the stomach. G. glabra extracts showed significant anti-ulcer activities in mice, attributed to its antioxidant / radical scavenging activities protecting tissues against radical / ROS damage and inflammation. Jalilzadeh-Amin et al, 2015
- May inhibit the adhesion of H. pylori to human stomach tissue. Both aqueous extracts (1 mg/mL) and polysaccharides from the roots of the plant are strong anti-adhesives and show cytoprotective effects. Wittschier et al., 2009.
- Glycyrrhizic acid in licorice can raise blood pressure when used on a frequent basis.
Encourage stomach lining to produce mucus. Reduces contact between stomach lining and stomach acid
- Eat Bananas
- Reduce stress
Avoid irritating foods / substances / triggers
- STRESS
- Alcohol
- Chocolate
- Spicy food
- Carbonated drinks
- NSAIDS / Aspirin
- Smoking
- Excessive regular salt
Regulate stomach acid
- Chewing gum increases acidity.
- Do not drink milk – The calcium and protein in milk stimulates the production of more acid.
Apple cider vinegar (ACV), baking soda and raw honey
- ACV and raw honey contain antioxidant polyphenols and kill H. Pylori with their antibacterial properties, all 3 ingredients have a healing alkalizing effect on body.
- Choose organic raw ACV with the mother (the stringy, gelatinous bits)
- Start with 2 tsp. ACV, add 1/2 tsp baking soda (let fizz), add 8oz water to dilute and drink consistently before meals. Gradually increase ACV dose to no more than 2 tablespooons.
- Note on ACV acidity: The acidity provided by a couple tablespoons of apple cider vinegar (ACV) isn’t going to “amount to a hill of beans” in altering the stomach’s acidity level



An ulcer cure using MELATONIN + B vitamins + amino acids
Formula used contains: melatonin (2.5mg), l-tryptophan (25mg), vitamin B6 (200mg), folic acid (10mg), vitamin B12 (50lg), methionine (100mg) and betaine (trimethylglycine)(100mg) in gelatin capsules taken ONCE / day. In the case history below, treatment lasted for 9 months. De Souza Pereira, 2006
melatonin inhibits gastric acid secretion and nitric oxide (NO) production.
Bubenik et al demonstrated that a 4-wk administration of melatonin in the diet significantly reduced the incidence of spontaneous gastric ulcers in young pigs. The ulcers in this case may have been due to a deficiency of melatonin synthesis.
Recently, melatonin (combined with other natural supplements) was successfully used to heal a patient with a giant ulcer of 6 cm (about 3.2 inches). This type of ulcer is typical of HIV positive patients. This patient took omeprazole and other PPIs prescribed by gastroenterologists for months. Neither treatment produced even partial relief of his symptoms. Subsequently, he started to lose weight because he could no longer eat properly because of the acute pain, impaired swallowing and massive hematemesis (Even when he tried to drink an apple blended with water he vomitted blood). As a consequence, he lost 40 kg in 6 mo. After he consulted five gastroenterologists, he was recommended to our research group. We prescribed him the above mentioned formula with melatonin, vitamins and amino acids. In 32 d of treatment, he regained 30 kg and the ulcer was (eventually) cured. [Pereira, 2006]
References
Asl MN, Hosseinzadeh H. (2008) Review of pharmacological effects of Glycyrrhiza sp. and its bioactive compounds. Phytother. Res. 22:709-24. PubMed Google Scholar
Atsushi et al (2010) Protective effects of a gastrointestinal agent containing Korean red ginseng on gastric ulcer models in mice; BMC Complement Altern Med. 10: 45. PubMed
Bae EA, Han MJ, Kim DH. (1999) In vitro anti-Helicobacter pylori activity of some flavonoids and their metabolites. Planta Med. 65:442-443. PubMed Google Scholar
Blankson H, Grotterød EM, Seglen PO. (2000) Prevention of toxin-induced cytoskeletal disruption and apoptotic liver cell death by the grapefruit flavonoid, naringin. Cell Death Differ. 2000;7:739-746. PubMed Google Scholar.
Brzozowski, Thomasz et al (2005) Grapefruit-seed extract attenuates ethanol-and stress-induced gastric lesions via activation of prostaglandin, nitric oxide and sensory nerve pathways. World J Gastroenterol. 2005 Nov 7; 11(41): 6450-6458. Published online 2005 Nov 7. PubMed Full text
Cianciosi, D et al (2018, Sep) Phenolic Compounds in Honey and Their Associated Health Benefits: A Review. Molecules; 23(9): 2322. PubMed
De Souza Pereira R. (2006) Regression of an esophageal ulcer using a dietary supplement containing melatonin. medicine published in J. Pineal Res. 2006 Semantic scholar (more detailed info)
Heggers JP, Cottingham J, Gusman J, Reagor L, McCoy L, Carino E, Cox R, Zhao JG.(2002) The effectiveness of processed grapefruit-seed extract as an antibacterial agent: II. Mechanism of action and in vitro toxicity. J Altern Complement Med. 2002;8:333-340. PubMed Google Scholar
Jalilzadeh-Amin, G., Najarnezhad, V., Anassori, E., Mostafavi, M., & Keshipour, H. (2015). Antiulcer properties of Glycyrrhiza glabra L. extract on experimental models of gastric ulcer in mice. Iranian journal of pharmaceutical research : IJPR, 14(4), 1163-1170. PubMed
Krausse R, Bielenberg J, Blaschek W, Ullmann U (2004) In vitro anti-Helicobacter pylori activity of Extractum liquiritiae, glycyrrhizin and its metabolites. J. Antimicrob. Chemother. 54 (1): 243-246. Oxford Journals
Mahady, Gail et al (2005, Nov) In Vitro susceptibility of Helicobacter pylori to botanical extracts used traditionally for the treatment of gastrointestinal disorders. Phytotherapy Research Volume 19, Issue 11, pages 988-991, Wiley
Motilva V, Alarcón de la Lastra C, MartÃn MJ. (1994) Ulcer-protecting effects of naringenin on gastric lesions induced by ethanol in rat: role of endogenous prostaglandins. J Pharm Pharmacol.;46:91-94. PubMed Google Scholar Ref list
Reagor L, Gusman J, McCoy L, Carino E, Heggers JP. (2002) The effectiveness of processed grapefruit-seed extract as an antibacterial agent: I. An in vitro agar assay. J Altern Complement Med. 8:325-332. Google Scholar
O’Leary, K. A., de Pascual-Teresa, S., Needs, P. W., Bao, Y. P., O’Brien, N. M., & Williamson, G. (2004). Effect of flavonoids and vitamin E on cyclooxygenase-2 (COX-2) transcription. Mutation research,551(1-2), 245-254. PubMed
Proteggente AR, Pannala AS, Paganga G, Van Buren L, Wagner E, Wiseman S, Van De Put F, Dacombe C, Rice-Evans CA. (2002) The antioxidant activity of regularly consumed fruit and vegetables reflects their phenolic and vitamin C composition. Free Radic Res. 36:217-233. Google Scholar
Sivam GP (2001 Mar) Protection against Helicobacter pylori and other bacterial infections by garlic. J Nutr. 131(3s):1106S-8S. PubMed
Torres J, Pereira R (2010, Oct) Which is the best choice for gastroesophageal disorders: Melatonin or proton pump inhibitors? World J Gastrointest Pharmacol Ther. 1 (5):102-106.Published online Oct 6, 2010. PubMed
Turco R, Martinelli M, Miele E, Roscetto E, Del Pezzo M, Greco L, Staiano A. Proton pump inhibitors as a risk factor for paediatric Clostridium difficile infection. Aliment Pharmacol Ther. 2010;31:754-759. PubMed
Wittschier N, Faller G, Hensel A. (2009) Aqueous extracts and polysaccharides from liquorice roots (Glycyrrhiza glabra L.) inhibit adhesion of Helicobacter pylori to human gastric mucosa. J Ethnopharmacol 125: 218-223. PubMed.
O.S. ZAYACHKIVSKA, S.J. KONTUREK, D. DROZDOWICZ, P.C. KONTUREK, T. BRZOZOWSKI, M.R. GHEGOTSKY. (2005) GASTROPROTECTIVE EFFECTS OF FLAVONOIDS IN PLANT EXTRACTS. JOURNAL OF PHYSIOLOGY AND PHARMACOLOGY56, Suppl 1, 219231 Semantic scholar pdf
Agudo S, Alarcon T, Urruzuno P, Martinez T, Lopez-Brea M. (2010) Detection of Helicobacter pylori and clarithromycin resistance in gastric biopsies of pediatric patients by using a commercially available real-time polymerase chain reaction after NucliSens semiautomated DNA extraction. Diagn Microbiol Infect Dis.67(3):213-219. PubMed Google Scholar
Agudo S, Perez-Perez G, Alarcón T, López-Brea M. (2010a) High prevalence of clarithromycin-resistant Helicobacter pylori strains and risk factors associated with resistance in Madrid, Spain. J Clin Microbiol. 48(10):3703-3707. PMC free article PubMed CrossRef Google Scholar
De Francesco V, Zullo A, Lerardi E, Vaira D. (2009) Minimal inhibitory concentration (MIC) values and different point mutations in the 23S rRNA gene for clarithromycin resistance in Helicobacter pylori. Dig Liver Dis. 41:610-611. PubMed CrossRef Google Scholar
Dial S, Alrasadi K, Manoukian C, Huang A, Menzies D. (2004) Risk of Clostridium difficile diarrhea among hospital inpatients prescribed proton pump inhibitors: cohort and case-control studies.CMAJ.171:33-38. PMC free article PubMed
Kalant H. Roschlau (1998) WHE Principles of Medical Pharmacology. 6th edition. New York: Oxford University Press; 1998. p. 558.
Vermeer IT, Engels LG, Pachen DM, Dallinga JW, Kleinjans JC, van Maanen JM.(2001) Intragastric volatile N-nitrosamines, nitrite, pH, and Helicobacter pylori during long-term treatment with omeprazole. Gastroenterology.121:517-525. PubMed
Viste A, Ovrebo K, Maartmann-Moe H, Waldum H. (2004) Lanzoprazole promotes gastric carcinogenesis in rats with duodenogastric reflux. Gastric Cancer. 7:31-35. PubMed
Drini M. (2017). Peptic ulcer disease and non-steroidal anti-inflammatory drugs.Australian prescriber,40(3), 91-93. doi:10.18773/austprescr.2017.037 Link










