Grave's Disease / Diffuse Toxic Goiter / Hyperthyroid
Characteristics of Grave’s Disease
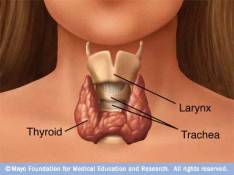
- Autoimmune stimulation of thyroid gland – antibodies against TSH receptors (TRabs) on thyroid follicular cell; binding to TSHR continuously activates the receptors in the absence of TSH, diffusely increasing follicular cell and follicle size and reproduction rate, leading to diffuse gland enlargement
- High T4 and T3 levels
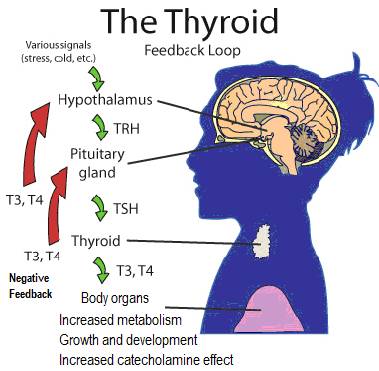
- Low TSH levels – as pituitary feedback compensates for high T4 / T3 by reducing its TSH secretion; this is the most sensitive measurement and the first obvious test for Grave’s.
- Causes hyperthyroidism – excess TH secretion can also lead to Thyrotoxicosis
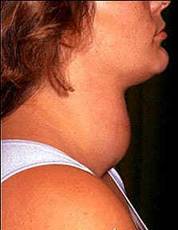
- Diffuse goiter usually present – slight or several times larger than normal
- Immune system lymphocyte presence
- Graves Ophthalmopathy in ~25% of cases – – some people have bulging eyes (Exopthalmos), eyelid retraction, inflammation in tissue surrounding eyes, double vision and sometimes even vision loss; may take years to heal.
- Spontaneous remission of hyperthyroidism in 30-40% of cases
- Pretibial myxedema in ~2% of cases – thickening skin with edema, painless lumps on lower legs
Risk factors
- 4-6 fold occurrence in women – compared to men
- Most often occurs in young, middle-aged adults – but can affect any age
- Genetic – increased risk in those with HLA-B8 allele.
Alternative Treatments
Low Dose Naltrexone could benefit some Grave’s cases – an interesting therapy against autoimmune diseases
High dose iodine to satisfy whole body sufficiency – Dr. Guy Abraham, MD, is foremost in the field with other medically qualified researchers into iodine supplementation for many thyroid disorders.