





Meet the immune system participants in the inflammatory process
| Immune System | I.S. | |
| White Blood Cells (aka leukocytes) | WBCs | Provide action against infection or injury |
| Extra-Cellular Matrix | ECM | Network of connective tissue, which fills spaces between cells, provides strength, binds cells and tissues together and links almost every cell in the body; |
| Cell surface Adhesion Molecule | CAM | Enables a cell to adhere to other cells or molecules in the ECM; specifically promotes adherence of WBCs (e.g. monocytes) to endothelium; includes Intercellular CAM-1 (ICAM-1), Vascular CAM-1 (VCAM-1), E-Selectin |
| Fibroblasts | Connective tissue cells that secrete precursors of all ECM components. | |
| Oxidative stress | A situation where reactive oxidants (i.e. free radicals) reactive oxygen species (ROS) and reactive nitrogen species (RNS) can cause damage to cells if there are insufficient antioxidants to control them. | |
| Antigen (antibody generator) | Ag | Our body recognizes an antigen as a foreign substance – such as pathogenic microbes, toxins from snake or insect bites and allergens (e,g, pollen) and other harmful particles. Our innate and adaptive immune systems promote the formation of an antigen-specific antibody. An antigen can bond to (i) an antibody antigen-binding site or (ii) a T-cell antigen receptor. Each T-cell antigen receptor has a specificity for a single antigen, in order to recruit only the lymphocytes required for that antigen. Antibody antigen-binding sites have the ability to “cross-react” to bind more than one antigen, Antigens exist on normal cells, cancer cells and/or microbes |
| Antibodies (immunoglobulins) | Ab | 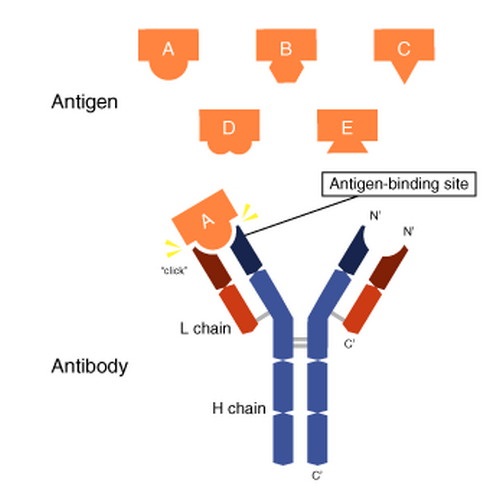 Used by the I.S. to identify and “tag” an antigen (particles, toxins, infected, damaged or cancerous cells) for removal by other parts of the I.S. Produced by B-cells, Abs are Y-shaped proteins belonging to the immunoglobulin family (IgA, IgD, IgE, IgG, IgM). The I.S. inserts antigen-specific Abs into the membranes of B-cells (specific to the same antigen). When armed with receptors (antigen-binding sites) at the tips of the Y of the Ab, they migrate to lymph nodes or the spleen. An antigen matching the Ab receptor, causes the B-cell to form the Mh2 complex, which it inserts into its plasma membrane. T-helper cells recognize the antigen Mh2 complex, which stimulates B-cell proliferation and differentiation into:
IgA – in tears, saliva, mucus, breast milk, intestinal fluid – protects against inhaled and ingested pathogens (organisms / microbes that can cause disease) |
| Endothelial cells | ECs | Endothelial cells form the endothelium – a single layer of squamous cells lining the interior surface of blood and lymphatic vessels, an interface between blood or lymph and the rest of the vessel wall. |
| Phagocytes | WBCs that engulf / ingest and destroy invading micro-organisms, cellular debris, and dead cells
Activated Neutrophils and macrophages produce reactive oxygen species (free radicals) – referred to as a respiratory burst. ROS chemically react with other substances to become potent microbicidal substances to add to the I. S. arsenal. | |
| Myelo-peroxidase | MPO | A lysosome (cell organelle that digests cellular waste inside and outside cell), most abundantly secreted from neutrophils, with oxidative stress being a factor. It proces hypochlorous acid from hydrogen peroxide. Contains heme (the green pigment seen in mucus and sputum). |
| Cytokines |
| |
| Granulocyte cells | Part of innate I.S. (1st line defense) characterized by so-called ‘specific granules’ in their cytoplasm (all material enclosed by cell membrane, except cell nucleus). Cell-killing molecules are released from granules when activated by an immune stimulus, in a process called degranulation.
| |
| Platelets | Modulate clot formation and have roles in inflammation, infection, immune response and cancer. Gather at damage site, adhere to WBCs, Subsequently release cytokines / chemokines, which are chemotactic for (i.e. mobilize) neutrophils and monocytes. Target lymphocytes, neutrophils and monocytes to inflammation sites, triggering further inflammation. Activated platelets release SEROTONIN (by degranulation). Causes itching ,and increases vasodilation vessel permeability. (SEROTONIN relates to muscular tone (TONIN) in blood (SERO) vessels) Platelets also engulf microbes. | |
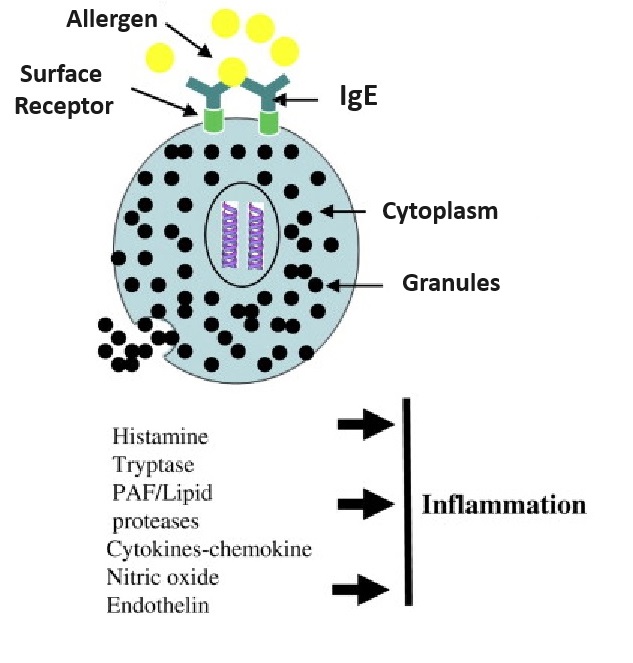
| Mast cells | MCs | Mast cells are your body’s alarm system – Key activists initiating the inflammatory process. These WBC granulocytes (made in bone marrow) are resident in connective and mucosal tissues (line membranes in body cavities, and cover organ surfaces). MCs are mostly present in and act upon tissues surrounding blood and lymphatic vessels, nerves, skin, urinary tract, mouth, conjunctiva, nose and numbers are elevated in and mucosa of asthmatic lungs, and GI tract of inflammatory bowel disease (IBS). MCs don’t destroy pathogenic invaders themselves, but “sound the alarm” for mediators to deal with the problem, creating inflammation, and then return the body to normal. Sometimes the immune system reaction can be over-zealous, mis-identifying a particle as a toxin, leading to such as seasonal allergies or allergic asthma. Mast cells are coated with a variety of receptors and quickly “sound the alarm” to protect tissue in their “neighborhood” against damage. They begin the inflammation process (in both the innate and adaptive immune response) when surface receptors are activated by physical injury or antigens, such as allergens, pathogenic microbes, harmful particles, toxins, venoms (e.g. from snake or insect bites), proteases, complement proteins, or chemical substances. When engaged by the appropriate ligand (E.g. LPS / Endotoxin of gram-negative bacteria, peptodoglycan of GRAM-POSITIVE BACTERIA), it triggers release of granules (by exocytosis), some discharging their inflammatory mediators immediately, others later.Mast cells are known for their role in allergies and anaphylaxis, but also have protective roles in wound healing (causes blood vessels to dilate allowing more blood and immune cells to reach damaged area), angiogenesis, pathogenic defense +++.Stimulus-specific mast cell mediators are released into the extracellular “neighborhood” – initiated by antigen or injury-activated MC surface receptors – these mediators either initiate inflammation or deal with the damage: |
- Released via mast cell degranulation:
- Histamine, in response to injury or toxic substance; increases vessel dilation / permeability, promoting blood flow to area and leakage of fluid, pathogen-fighting WBCs and proteins from blood into the tissue space. This causes redness, warmth, swelling, itching and pain.
- Heparin (an anticoagulant),
- Serine proteases (e.g. trytase, chymase),
- Myeloperoxidase enzyme (MPO) – most abundantly by neutrophils. Can oxidize LDL in the space just below the endothelium.
- Mast cells synthesize (de novo):
- Eicosanoids (lipid signaling factors) from membrane omega-6 arachidonic acid. Consuming a balance of both inflammatory (most omega-6 fats) and anti-inflammatory omega-3 EPA and DHA, and omega-6 GLA) fatty acids will ensure a balanced response when dealing with injured tissue; EFAs ==> Local Hormones – First Response Team
- Prostaglandin D2 (PGD2) – bronchoconstricting, pivotal roles in antigen presentation, leukocyte activation, ECM deposition, fibrosis.
- Leukotriene B4 (LTB4) – chemoattractant for neutrophils
- Leukotriene C4 (LTC4)
- Chemoattractants (E.g. chemokines, cytokines) – which attract leukocytes (white blood cells) to the “scene of the crime”. Large amounts of TNF-α released by stimulated mast cells as a result of pathogen exposure.
- Chondroitin sulfate
- Mast cells (and basophils) cause formation of bradykinin (BK) (by releasing heparin)
- The bradykinin receptor B1 is expressed only as a result of tissue injury. BK (produced from an inactive precursor always circulating in the blood) is released from mast cells and basophils,
- Dilates blood vessels / lowers blood pressure (by stimulating NITRIC OXIDE and increases blood vessel permeability. To allow needed blood components to enter the tissue space; ACE inhibitor drugs reduce blood pressure by increasing bradykinin.
- Contracts airway smooth muscle and is a potent bronchial vasodilator, stimulates mucus secretion and coughing. BK activates release of neuropeptides from sensory nerves in airways, leading to reflex bronchoconstriction, coughing and neurogenic inflammation. Fuller RW, Dixon CM, Cuss FM, Barnes PJ. Bradykinin-induced bronchoconstriction in humans. Mode of action. Am Rev Respir Dis. 1987 Jan;135(1):176-80. PubMed
- Effects produce redness, warmth and swelling and is Involved in pain mechanism
- Stimulates phospholipase. Increases the production of prostaglandins (local “hormones”)
These mediators recruit all types of white blood cells to the site, many of which are activated to produce their own inflammatory mediators. Types of white blood cells recruited include:
- Monocytes. Become macrophages (“big eaters”) when they leave the blood and enter the tissue
- Neutrophils. Squeeze through capillary walls and into infected tissue to kill invaders and then engulf the remnants by phagocytosis.
- Antigen-presenting dendritic cells. Main function is to process antigen material and present it on the cell surface to the immune system’s T-cells, thereby acting as messengers between the innate and the adaptive immune systems).
- All kinds of lymphocytes:
- Natural Killer (NK) cells. Specialized to kill certain types of target cells (esp. virally infected or cancerous host cells) in innate (1st line of defense) immunity
- B-cells and T-cells. These cells lead to an adaptive immune response (2nd line of defense which “remembers” that the problem has happened before and is prepared for it);
- Eosinophils. Blood levels increase sharply with parasitic worm infections. Eosinophils release the cytoxic contents of their granules on the “invader”.
Matrix metallo-peptidase-9MMP-9MMP-9 is one of the matrix metalloproteinase enzymes that degrade ECM proteins and can degrade the fibrous cap on plaque. MMP-9 digests ECM decorin, elastin, fibrillin, laminin, gelatin (denatured collagen), and collagen types IV, V, XI and XVI; MMP-9 levels are elevated during inflammation in CHD, arthritis, pulmonary-emphysema, diabetic retinopathy;Lymphocytes
Small WBCs of the ADAPTIVE I.S.
- T-cells – “Killer” (cytotoxic) T-cells directly kill infected, damaged, or cancer cells presenting antibodies on cell surface used to “tag” problem cells; “Helper” T-cells – release cytokines, further activating killer T-cells and memory B=cells
- B-cells. Make antibodies in response to antigens and abnormal cells (e.g. cancer cells). Two types:
- Plasma cells: produce / release Abs in response to antigens
- Memory cells: remember particular antigens for future defense if pathogen returns
Large granular WBCs of the INNATE and ADAPTIVE I.S.
- NK-cells (natural killer cells) – similar to “Killer” T-cells, quickly responds to and kills infected, damaged, cancer cells, especially highly proliferative cells, Unlike “killer” T-cells which need a cells to be “tagged”, NK-cells recognizes them via cell-mediated immunity ( i.e. without detecting antibody presence), based on activating and inhibitory receptors, and kills pathogens by secreting cytotoxic granules
Acute phase proteins (APPs)
In response to infection or trauma, APPS are expressed by most cells – including activated endothelial cells (ECs), mast cells and macrophages, and used in cellular communication to modulate cell growth, development, repair, fibrosis, inflammation, immunity and other processes to maintain body in a steady state; Blood plasma concentrations of specific APPs, called acute-phase reactants (APRs), will either increase or decrease in response to inflammation.
ACUTE-PHASE REACTANTS (APRS)
Most produced by liver (some by other cell types, including monocytes, ECs, fibroblasts and adipocytes)
SOME APRS INCREASE DURING INFLAMMATION (CALLED POSITIVE ACUTE-PHASE APRS)
For example:
- C-reactive protein (CRP) – not normally present in blood, a reliable risk-marker of inflammation / atherosclerosis.
- Activates the complement system (immune system defense mechanism) to opsonize (add a negatively charged coating to) microbes in preparation for their destruction.
- Enhances phagocytosis of low-density lipoprotein, leading to the formation of foam cells;
- Data suggests CRP may increase CAM expression.
- Complement factors – complex series of protein molecules circulate in the plasma and other extracellular fluids in an inactive form. Enzymes convert complements into biologically active molecules when exposed to microorganisms or other foreign substances to destroy or mark cells for destruction
- Coagulation factors. Fibrinogen, prothrombin, plasminogen.
OTHER APRS DECREASE DURING INFLAMMATION (CALLED NEGATIVE ACUTE-PHASE APRS)
- Albumin
- Transferrin
- Anti-thrombin – decreasing it allows blood to clot
- Retinol-binding proteins.









