NSAIDS (Cox enzyme inhibitors / Coxibs) - Anti-inflammatory drugs WARNING!
NSAIDS are taken to relieve pain and inflammation
The traditional, better-known NSAIDS (Non steroidal anti-inflammatory drugs) include aspirin (Beyer®), ibuprofen (Motrin®, Advil®), and naproxen (Aleve®). Acetaminophen (Tylenol) is not an NSAID – it reduces fever and pain but not swelling / inflammation).
The usual purpose of NSAIDs is to reduce inflammation and associated pain by inhibiting the COX-2 enzyme, which would otherwise produce mostly inflammation-promoting prostanoids from omega-6 arachidonic acid (AA) fatty acids in cell membranes. Prostanoids are a subgroup of eicosanoids (all produced from the essential omega-3 and omega-6 polyunsaturated fats), which predominately have the effect of promoting inflammation with its associated pain, blood-clotting and cell proliferation. Eicosanoids act as hormones in local areas of trauma / infection, ALL vitally involved in mediation of:
| Inflammation / allergies | Regulating blood pressure & clotting |
| Regulating immune responses & function | Providing gastroduodenal lining protection & integrity |
| Reproduction (ovulation and implantation) | Angiogenesis (development of new blood vessels — vital for cell growth but can also spread cancer). |
For the general effects of the different eicosonoids:
Cox-1 and Cox-2 enzymes
The conversion from essential fatty acids to eicosanoids is via two key enzymes COX-1 and COX-2.
The traditional NSAIDs, such as Beyer®, Motrin®, Advil® and Aleve® inhibit both of these enzymes, preventing both the inflammatory and anti-inflammatory functions of eicosanoids.
COX-1 is always present at low levels in tissues doing housekeeping and maintaining homeostasis, while COX-2 is only induced by appropriate physiological stimuli (cytokines, tumor promoters and growth factors) after tissue damage, infection, allergic reaction or in development of cancer. Thus, inhibiting both COX-1 and COX-2 does reduce inflammation and pain, but it also inhibits the production of eicosanoids with their beneficial functions as seen in the Chart of significant effects of eicosanoids, with sometimes deleterious health consequences. E.g. in stomach and duodenum, it removes protection for the stomach and intestinal lining and thereby sets the stage for ulcers.
COX enzymes operate in particular locations.
COX-1 operates in the gastrointestinal lining (GI mucosa).
COX-1 activity is responsible for producing cell-protective prostaglandins, such as prostacyclin (PGI2) and PGE2, critical for maintaining integrity of gastric mucosa.
COX-2 is overexpressed in 50% of benign polyps and 80-85% of adenocarcinomas.
Risks of severe complications using cox-1 inhibitor NSAIDs
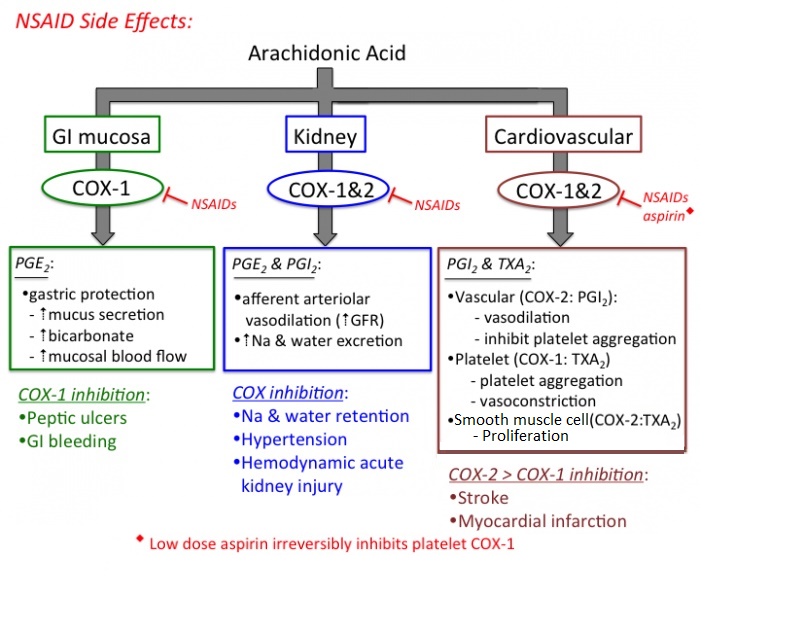
The above diagram only considers the prostanoids, but COX-1 enzyme inhibitors affect functions of the other eicosanoids too.
COX-1 inhibitors include aspirin, Aleve, Advil and Motrin
Use of cox-1 inhibitor NSAIDs significantly increases risk of death. Unfortunately, when NSAIDs block the COX-1 enzyme the body loses some important functions provided by this enzyme Including:
- Maintaining the integrity of mucosal cells lining the stomach and intestines. Thereby promoting stomach and duodenal ulcers
- Helping maintain kidney function.
- Promoting blood clotting. Low dose aspirin is largely used as a prevention for CVD and heart attacks. However, there is some evidence that concurrent use with other NSAIDS, which generally do not have this CVD prevention benefit, may inhibit aspirin’s antiplatelet effect. Effects of cox-1 inhibitor NSAIDS maintained throughout the 10-day life of the platelet.
The loss of such protective functions easily explains the unwanted side-effects of using COX-1 inhibiting NSAIDs. In fact, extended use of COX-1 inhibiting NSAIDS can cause GI discomfort and stomach ulcers leading to internal bleeding. A 2000 analysis including data of 250,000 patients from 15 randomized clinical trials, found that, on average, one of 1220 patients who take NSAIDs for at least two months will die as a result of gastroduodenal complications. This presents a pretty significant risk of dying! — In perspective, it is 1000 times more perilous than taking a single flight. Number Needed To Kill Individual Drug Risk with NSAIDs, 2001 And to hammer home this alarming risk — comparing data published from pre-1997 to that from 1997-2008, mortality in patients suffering from an upper gastrointestinal bleed or perforation has fallen from 1 in 9 to 1 in 13 overall, but has actually increased from about 1 in 7 to 1 in 5 in those exposed to NSAIDs! Straube et al, 2009
Selective COX-2 inhibiting NSAIDs
In light of problems caused by inhibiting COX-1, some newer NSAIDS selectively block only the COX-2 enzyme.
- Celecoxib (Celebrex®)
- Obscenely expensive Rofecoxib (Vioxx®, recalled in 2004) was an attempt at suppressing COX-2, whilst preserving COX-1. It FAILED, causing an estimated 60,000 deaths due to heart attack or stroke.
However, selective COX-2 inhibitors ONLY HALVE the incidence of serious gastrointestinal events seen with COX-1 inhibitors. This may partially reflect their impact on epithelial COX-2–dependent prostaglandins and thromboxane that accelerate ulcer healing in the stomach and intestinal duodenum.
NOTE: unlike aspirin, COX-2 inhibitors are not effective for preventing strokes or heart-attacks in individuals at high risk for such.
Alternative anti-inflammatory treatments
Salicylates – promising anti-inflammatory drugs (also lower blood sugar)
- Do not affect the Cox enzymes at all but instead inhibit the master factor in inflammation called NF-kB. This is activated in response to stress, cytokines [E.g. TNF, IL-1b], free radicals, UV radiation, ionizing radiation, oxidized LDL, bacterial / viral infections, cocaiine);
- Generic form called salsalate is better tolerated than sodium salicylate
- Salicylates not only reduce inflammation, but they also lower blood glucose.
In 2013, researchers published results of stage 2 of a clinical trial called TINSAL-T2D (Targeting Inflammation using salsalate in Type 2 Diabetes), which involved 286 participants who could not adequately control their blood sugar levels with medication. 48 weeks of treatment lowered HbA1C by 37% more than placebo group. Goldfine et al, 2010
NATURAL, SELECTIVE COX-2 Inhibitors
- Many phytonutrients contain selective COX-2 inhibitors – including, amongst many others:
- Polyphenols (anthocyanins) in cherries
- Curcumin in curries and yellow mustard (not brown or Dijon)
Phytonutrients – Anti-inflammatory, Antioxidant and/or Anticancer
Acetaminophen (E.g. Tylenol®) is a pain-killer, not an anti-inflammatory drug
- Acetaminophen, although not an NSAID, also inhibits prostaglandin synthesis, but is less likely than NSAIDs to increase blood pressure or cause stomach pain / bleeding. However, it may cause liver damage / failure, especially at high doses. Additionally, it can increase the anti-blood-clotting effect of the blood-thinner warfarin.
Anti-inflammatory tactics
How to moderate eicosonoid/prostanoid effects
How to treat CHRONIC Inflammation
How to treat ACUTE (Short-lived) Inflammation
References
Antman EM, Bennett JS, Daugherty A, Furberg C, Roberts H, Taubert KA. (2007) Use of nonsteroidal anti-inflamatory drugs: an update for clinicians: a scientific statement from the American Heart Association. Circulation 2007; 115 (12): 1634-42. Circulation
Goldfine AB, Fonseca V, Jablonski KA, Pyle L, Staten MA, Shoelson SE (2010 Mar 16) The effects of salsalate on glycemic control in patients with type 2 diabetes: a
randomized trial Ann Intern Med 152(6):346-57 PubMed
S.Straube et al (2009 Jun 5) Mortality with upper gastrointestinal bleeding and perforation: effects of time and NSAID use. ;BMC Gastroenterol. 9:41. PubMed
Number Needed To Kill Individual Drug Risk with NSAIDs Tramèr MR, Moore RA, Reynolds DJM, McQuay HJ (2000) Quantitative estimation of rare adverse events which follow a biological progression – a new model applied to chronicNSAID use. Pain 85:169-182 Link