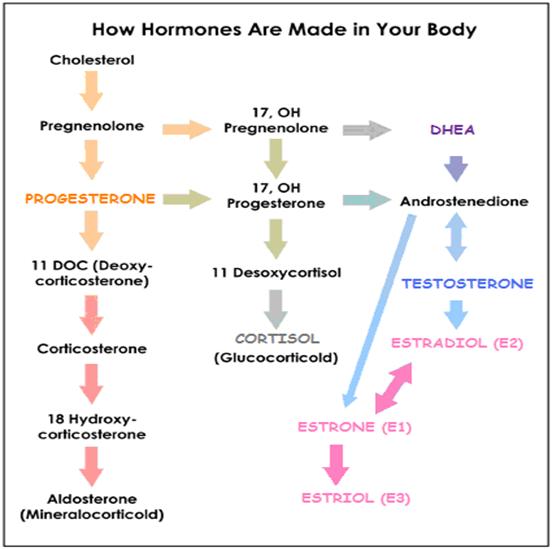
PROGESTERONE Supplementation Dosage Chart

*** FIRST*** – Please read: Estrogen dominance treatment
The best delivery routes and methods for PROGESTERONE cream / gel are:
- Women. Via the vaginal epithelial membranes, using cream or suppositories
- Men.
- (Via the rectal epithelial membrane using suppositories
- or Rubbing cream into clean/dry testicles. Note: PROGESTERONE has no feminizing characteristics
The following chart gives guidelines for PROGESTERONE cream dosage – when using vaginal or rectal suppositories, use the same suggested number of mg of PROGESTERONE given in the chart.
For women, “Day 1” in the chart refers to the first day of your period (if you are still menstruating)
PROGESTERONE Cream Dosage Chart(see special cases below) ¼ tsp. of ~1.6% cream contains ~20mg PROGESTERONENOW™ brand Natural PROGESTERONE cream contains 1.3g PROGESTERONE in 85g (3oz) cream = 1.53% | |||
Who /What Condition? | 1.6% Prog. Cream Amount | DAYS* From-To | Comments |
| Premenopausal women with PMS / Estrogen dominance symptoms (including fibrocystic breasts and ovarian cysts) *Ovulating* | 1/8 tsp. (10mg) | Twice daily Day after ovulation* for 14 days | *To figure PROGESTERONE start date, count back 14 days from when your next period is due (Day 1). Alternatively, use a fertility monitor to accurately ascertain when you ovulate. Family Planning Tools Fibrocystic breasts. Breast tissue usually returns to normal within 3-4 months. Then reduce the dose. |
| Premenopausal women with PMS / Estrogen dominance symptoms (including fibrocystic breasts and ovarian cysts) *Not Ovulating* | 1/8 – 1/4 tsp. (10-20mg) | Twice daily Begin on: Calculate Start Date*for 14 days | *To figure PROGESTERONE start date, count back 14 days from when your next period is due (Day 1). Allow 7 days off whether or not menstruation occurs, before beginning again; abrupt lowering of PROGESTERONE levels is the primary stimulus for menstruation to start. Hopefully, period pain and PMS will be dramatically reduced. Use indefinitely; |
| Aid conception / Prevent miscarriage | PROGESTERONE for Conception and Pregnancy problems related to Luteal Phase Deficiency (LPD) | ||
| Peri-menopausal women | 1/8 – 1/4 tsp. (10-20mg) | Twice daily Days 12 – 26 | |
| Menopausal / Post-menopausal women (who have not had a hysterectomy) | 1/4 – 1/2 tsp. (20-40mg) | Twice daily For 3 mths; | 25 days/month, then 5 days off; • If experiencing hot flashes or other menopausal symptoms during the days off, reduce the time off to 2-3 days for several months and then experiment with extending the days off back to 5 or 6. • If using supplemental estrogen, use PROGESTERONE every day of the month. |
| then1/4 tsp. (20mg) | Twice daily | ||
| For women who have had a complete hysterectomy (removal of both ovaries and uterus) or surgical menopause | First 2 months after surgery:1/4 tsp (20mg) at bedtime. Then reduce to 1/8 tsp (10mg) | Daily 25 days of calendar month | |
| Endometriosis | 1/4 tsp (20mg) in a.m. 1/2 tsp. (40mg) at bedtime | Days 8 thru 26-30 (End of your normal cycle) | Can take up to 6 months to control symptoms – once the outbreaks of endometriosis are tolerable reduce usage to days 12 till menstrual cycle. If you are too sleepy with high dose of PROGESTERONE, reduce the dose until the sleepiness goes away. |
| Osteoporosis Prevention | 1/8 – 1/4 tsp (10-20mg) | 12- last day of cycle | Use indefinitely, post-menopausal use calendar month instead of cycle |
| Osteoporosis Treatment | 1/2 tsp. (40mg) am/pm Then 1/4 tsp. (20mg) am/pm | 12 days until improve | Also supplement calcium (1g), magnesium, zinc, boron, manganese, vitamins D and K. If bone scans show improvement, you can reduce dose in half again. PROGESTERONE against Osteoporosis |
| PCOS | 1/4 tsp. (20mg) | Days 14 thru 28 | Adjust for a shorter or longer cycle |
| Uterine Fibroids | 1/4 tsp. (20 mg) | P.M. Days 8, 9, or 10 thru 26-30 (End of your normal cycle) | Continue until menopause, then reduce dose |
| Vaginal atrophy | 1/4 tsp. (20 mg) | P.M. | Apply together with vitamin E at bedtime |
| Chronic Fatigue | |||
| BPH / Prostate cancer | 1/8 tsp. (10mg) | A.M. and P.M. | Daily application to rectum or cleaned scrotums (testicles) to get it into prostate receptors; shown to reduce prostate size/BPH, normalize PSA levels, reverse prostate cancer, decrease urinary / frequency; Consider PROGESTERONE ‘therapy if over 40 with family history of prostate cancer or BPH; PROGESTERONE’s inhibitory effect on 5α-reductase is more effective than Proscar (finasteride – the standard 5α-reductase inhibitor medical cure for BPH) |
| Men (Estrogen dominance and over the age of 40) | 1/16+ tsp. (5-8 mg) | A.M. and P.M. until improve | Daily application to cleaned scrotum area; prevents osteoporosis in men, physiological doses appear to enhance sexual drive; may decrease male balding; may provide relief from pain / swelling of RA when rubbed in joints. For osteoporosis use indefinitely |

Special Cases
Some “Special Case” women need an initial 2-3 month LOADING dose
In any of the following situations Dr. John Lee recommended a higher dose of PROGESTERONE in the first 1-2 months of using PROGESTERONE cream – to help to replenish the depleted PROGESTERONE stores in the body’s fat. After a couple months the dose can be lowered to the usual dosage.
- Women who have had many months or years of cycles with no ovulation, which can create extreme PROGESTERONE deficiency – Each cycle that passes without ovulation can increase estrogen dominance as PROGESTERONE stores are depleted.
- Very thin women – who have little body fat can become estrogen dominant very easily as there is no fat to store extra PROGESTERONE .
- Women with PMS – You need a higher dose of PROGESTERONE for the first month or two because of the high CORTISOL level competing with PROGESTERONE
LOADING dose: 1/4 teaspoon 2x daily (Total 40mg / day) for two weeks before your period
Regular dose: 1/8 teaspoon 2x daily (Total 20mg / day) for two weeks before your period
Women using estrogen supplements
Dr. Lee had the opinion that there is no reason for a woman who is still menstruating to take estrogen – if you supplement PROGESTERONE , then reduce your estrogen dose by half and gradually taper off it completely.
Using PROGESTERONE for conception and/or to prevent miscarriage
PROGESTERONE for Conception and Pregnancy Problems related to Luteal Phase Deficiency (LPD)











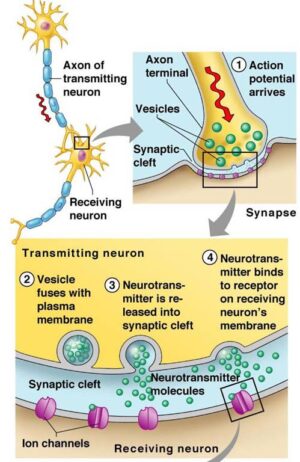
![<span class="ACETYLCHOLINE">Acetylcholine (Ach)</span><span class="hdg-smaller"> – Movement, memory, learning neurotransmitter</span> – [Cloned #60543]](https://healthhappening.com/wp-content/uploads/2025/12/Ach.jpg)