















Vitamin B12 (Cobalamin) - "The energy vitamin"

Introduction to B12
B12 is the largest molecule of all the vitamins. Also has a complex structure. B12 is unique among the vitamins containing a metal ion (cobalt). Explaining its name
In mammals, B12 is a cofactor for 2 enzymes:
- Methione synthase. Required for synthesis of amino acid methionine from homocysteine (elevated levels involved in CVD), which is itself needed for synthesis of SAME ( methyl group donor for methylation reactions, including methylation of DNA)
- L.methylmalonyl- CoA mutase. Instrumental in producing energy from fats and proteins, and in synthesis of hemoglobin (carries oxygen in RBCs)
B12 found in significant amounts in animal foods, but neglible amounts in plant food
This antioxidant vitamin has many functions in the body
B12 has beneficial functional roles in:
- Maintaining energy levels involved in metabolizing carbohydrate and fats
- Neurological function / mental alertness / Stress
- Homocysteine levels for healthy cardiac function
- Insomnia
- Cell growth / repair
- Immune function
B12 health benefits – include:
- Help folic acid form red blood cells
- Helps body utilize iron
- Aids neural function/ communication; helps maintain neural sheath protecting nerves
- Involved in adrenal hormone production
- Required for MELATONIN production
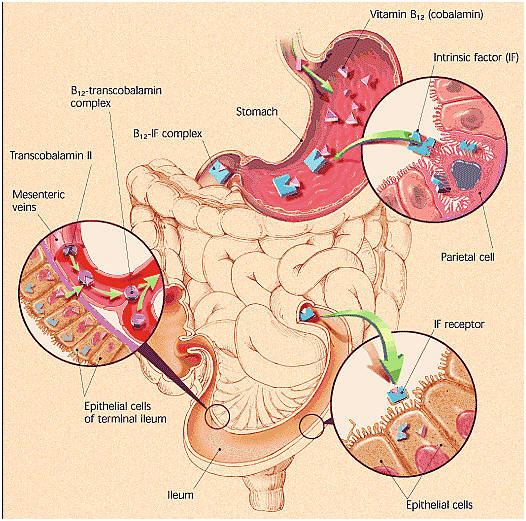
B12 absorption “journey” in the body
- Stomach acid and the protease enzyme pepsin frees B12 from food. The free B12 then binds to an R protein (haptocorrin), a glycoprotein released from the salivary glands and gastric mucosa.
- Pancreatic enzymes again release the B12 from R protein in the less acidic small intestine (duodenum). Allowing the free- again B12 to bind to intrinsic factor (IF), which was secreted by parietal cells of the stomach lining (gastric mucosa)
- After traveling to the ileum, intestinal lining receptors take up B12-IF complex. There its B12 is endocytosed by epithelial cells bound to transcobalamin to enter the liver, but only if calcium is present (supplied by the pancreas)
- Alternatively, B12 can be absorbed via the intestinal lining of the terminal ileum. By passive diffusion into the mesenteric veins, but this route has a very inefficient 1% absorption rate
Carmel R. Cobalamin (Vitamin B12). In: Shils ME, Shike M, Ross AC, Caballero B, Cousins RJ, eds. Modern Nutrition in Health and Disease. Philadelphia: Lippincott Williams & Wilkins; 2006:482497.
- B12 is stored in the liver for about 1 – 5 years. Depends on amount consumed, amount absorbed and hepatic function B12
B12 deficiency is not uncommon and often goes unrecognized
Some misdiagnosed diseases may simply be a B12 deficiency which has been referred to as a “silent epidemic”. Symptoms of B12deficiency can parallel those of several diseases, misleading doctors to misdiagnosis of M.S., Alzheimer’s, dementia, early Parkinson’s disease, diabetic neuropathy, chronic fatigue syndrome and more.
Sally M Pacholok, Jeffrey J Stuart, Could it be B12? An Epidemic of Diagnoses 2nd Edition Feb 2011
A B12 deficiency needs to be timely addressed, since it can result in permanent damage due to neuronal demyelination and axonal degeneration (called Wallerian degeneration results from insult to peripheral nerve fibers),which if left untreated will result in neuronal death.
Serum levels of B12 below 221 pmol/L (300 pg/mL) is the generally accepted level suggesting a tissue level deficiency
Rajan S, Wallace JI, Beresford SA, et al. Screening for cobalamin deficiency in geriatric outpatients: prevalence and influence of synthetic cobalamin intake. J Am Geriatr Soc, 2002;50:624630.
B12 deficiency is commonly related to:
- Food. Cobalamin malabsorption syndrome (MOST COMMON REASON) – occurs when the stomach lining loses the ability to produce intrinsic factor, a protein that binds to B12 to enable its absorption whenit reaches the lower end of the small intestine;
- You can be consuming B12 in animal products and still not be absorbing enough of it
- Those over the age of 50 have limited ability to absorb B12
- Pernicious Anemia. Progressive automimmune destruction of stomach lining cells:
(1) Reduces secretion of B12– releasing gastric acid and enzymes
AND
(2) Antibodies bind to intrinsic factor preventing formation of B12– IF complex and consequently B12 absorption.
Intramuscular B12 shots are a common treatment, although high dose oral B12 delivers similar amounts (E.g. 1000mg supplies 1 mg B12 by passive absorption) .
Kuzminski AM, Del Giacco EJ, Allen RH, Stabler SP, Lindenbaum J. Effective treatment of cobalamin deficiency with oral cobalamin. Blood. 1998;92(4):11911198. (PubMed)
Lederle FA. Oral cobalamin for pernicious anemia. Medicine’s best kept secret? JAMA. 1991;265(1):94-95.
Hathcock JN, Troendle GJ. Oral cobalamin for treatment of pernicious anemia? JAMA. 1991;265(1):96-97.
- Food-bound vitamin B12 malabsorption. More common in those over 60 commonly resulting from atrophic gastritis, in which atrophy of stomach glands results in stomach inflammation (possibly associated with H. Pylori)and decreased stomach acid production, and thus nonrelease of B12 from food. This is different to pernicious anemia because intrinsic factor is still available, which means that crystalline-form B12 in supplements or fortified food, which is not bound to protein, can still be absorbed.
Aging. Typically because of dietary insufficiency or malabsorption. Hydrochloric acid (HCl) is needed to release B12 from food, but HCl production decreases with age and HCl levels are decreased by long-term use of antacids or anti-ulcer drugs.
20- 50% of those over 50 are unable to absorb natural (protein-bound) B12
Institute of Medicine. Dietary reference intakes for thiamin, riboflavin, niacin, vitamin B6, folate, vitamin B12, pantothenic acid, biotin and choline. Washington, DC: National Academy Press 1998.
- AIDS. Increases risk of B12 deficiency, possibly due to failure of IF-B12 receptors to take up IF-B12 complex
Shane B. Folic acid, vitamin B12, and vitamin B6. In: Stipanuk M, ed. Biochemical and Physiological Aspects of Human Nutrition. Philadelphia: W.B. Saunders Co.; 2000:483518.
- Vegan diet. Animal products are the prime B12 source; predominantly vegetarian cultures (E.g. India) have high B12 deficiency rates.
- Surgical resection of ileal intestine containing IF- B12 receptors
- Pancreatic insufficiencies of enzymes or calcium
- Those taking Metformin. May interfere with absorption of calcium, required for small intestine receptors to take up B12
Herbert V. Vitamin B12. In: Ziegler EE, Filer LJ, eds. Present Knowledge in Nutrition. 7th ed. Washington D.C.: ILSI Press; 1996:191205.
Symptoms of B12 deficiency include:
- Megaloblastic anemia. Diminished folate production, even in the presence of folate; a symptom of pernicious anemia; produces large, immature, hemoglobin-poor RBCs
- Neurological. Numbness/tingling in arms, or legs, difficulty walking, memory loss, disorientation, dementia, possibly due to megaloblastic anemia or nerve sheath damage
- GI-related symptoms – sore tongue, loss of appetite, constipation
Some diseases associated with B12 deficiency
Reference: Linus Pauling Institute
- Cardiovascular Disease (CVD) related to elevated homocysteine levels
- Cancer related to deficiency of folate and its connection to DNA synthesis
- Neural tube defects – possibly connected to folates role in reducing homocysteine, since increased risk of NTD is associated with elevated levels of homocysteine
- Alzheimer’s disease / Dementia – possibly connected to B12‘s role in myelin sheath integrity
- Depression
RDA for adult men and women is 2.4 mcg B12 / day
Absorption or retention rate is related to the dose provided
Institute of Medicine. Dietary reference intakes for thiamin, riboflavin, niacin, vitamin B6, folate, vitamin B12, pantothenic acid,biotin and choline. Washington, DC: National Academy Press 1998.
| Dose Synthetic B12 | Delivery Method | Absorption Rate |
|---|---|---|
| (i.e. Non- protein bound) | ||
| < 5 μg | Oral (w/ non- deficiency) | 50-60% |
| >500μg | Oral (w/ non- deficiency) | 1% |
| <40 μg | IM | 93-100% |
| 1000 μg | IM | 15% |
Natural B12 Sources
Only bacteria can make B12 – such that B12 is naturally present bound to protein in fish, animals and their products, but not significantly in plants (unless they still have dirt on them). In this form, B12 must first be cleaved from protein via stomach acidand pepsin to be available for absorption.
| Food | Serving | Vitamin B12 (mcg) |
|---|---|---|
| Clams (steamed)* | 3 ounces | 84.0 |
| Mussels (steamed)* | 3 ounces | 20.4 |
| Crab (steamed)* | 3 ounces | 8.8 |
| Salmon (baked) | 3 ounces | 2.4 |
| Beef (cooked) | 3 ounces | 2.1 |
| Nutritional yeast | 1 T flakes | 2.1 |
| Milk (whole, 3.25%) | 1 Cup | 1.1 |
| Yogurt (Plain, lowfat) | 4 ounces | 0.75 |
| Egg (poached) | 1 large | 0.6 |
| Brie (cheese) | 1 ounce | 0.5 |
| Chicken (roasted) | 3 ounces | 0.3 |
| Turkey (roasted) | 3 ounces | 0.3 |
*There’s a reason for the high B12 values in shellfish i.e. a high bacterial load!
Who needs to supplement B12?
Non-vegan diet for healthy people should provide sufficient B12. However, the following persons should definitely supplement B12
- Strict vegetarians
- Women intending to get pregnant
It is prudent for those with conditions related to B12 malabsorption to empirically supplement B12 (especially given the lack of reliable diagnostic tests together with the low risk of B12supplementation)
- The “Over 50’s”
- Those who have had:
- Bariactric surgery
- Ileal resection of >20cm
- Partial or total gastrectomy may damage/remove parietal cells responsible for gastric acid production
- Those with:
- Low stomach acid. Usually due to atrophic gastritis caused by H. Pylori infection, common in over 50’s). Need B12 in supplemental (non-protein bound) form since they can not depend on hydrochloric acid to cleave B12 from food.
- Pernicious anema. Due to lack of gastric acid and intrinsic factor; those with pernicious anemia need a high dose B12 supplement that relies on the 1% B12 absorption by passive diffusion at the terminal ileum (where the small intestine meets the colon). E.g. Crohn’s disease, Celiac’s disease
- People with chronic alcoholism. Due to atrophy of the villi in the small intestines. Lambert D, Benhayoun S, Adjalla C, et al. Alcoholic cirrhosis and cobalamin metabolism. Digestion, 1997;58:64- 71.
- Whipples Disease. Causes malabsorption
- Chronic pancreatitis. Insufficient pancreatic secretions impedes cleavage of B12 from B12Rprotein complex, and therefore formation of the B12IF complex. Andres E, VidalAlaball J, Federici L, et al. Clinical aspects of cobalamin deficiency in elderly patients. Epidemiology, causes,clinical manifestations, and treatment with special focus on oral cobalamin therapy. Eur J Intern Med, 2007;18:456- 462.
- Small intestine bacterial overgrowth. Bacteria bind B12 for their own use; at risk are those with hypochlorhydria, intestinal dysmotility, intestinal obstructions or adhesions, intestinal diverticuli, blind loops of bowel due to past surgery, and those without an intact ileocecal valve.
- People taking meds that interfere with B12 absorption:
- Gastric acid suppressive agents. i.e. proton pump inhibitors (E.g. omeprazole, lansoprazole), H2inhibitor antagonists (E.g. Tagamet, Pepsid, Zantac);
- Cholestyramine (anti-cholesterol)
- Neomycin (antibiotic)
- Colchine (anti- gout)
- Metformin (diabetic med) (ties up needed calcium)
- Nitrous oxide (laughing gas) (anaesthetic) inhibits B12-dependent enzymes
- Also those with cirrhosis. Diminishes liver’s storage capacity of B12; Paradoxically, a degrading liver causes high serum B12 as it releases its stores, although despite raised serum levels, the tissues remain depleted. Ermens AAM, Vlasveld LT. Significance of elevated cobalamin (vitamin B12) levels in blood. Clin Biochem, 2003;36:585590.
Supplementing B12
Which is the best form of B12 supplement?
There are 3 forms of B12 to choose from found in supplements and fortified foods:
- Hydroxycobalamin
- Cyanocobalamin (popular form in supplements). Produced from hydroxocobalamin, the form produced by bacteria;
- Methycobalamin (BEST, “Ready- to- go”, physiological form). Natural form produced in the body from bacterial hydroxycobalamin;
Delivery methods
There are 3 main delivery methods for B12 i.e. Injection (IM), oral tablets or sublingual tablets or drops. Study showed that all 3 methods have an equal affect at correcting B12 deficiency (study participants’average serum B12 was 100 pmol /L)
Delpre G, Stark P, Niv Y. Sublingual therapy for cobalamin deficiency as an alternative to oral and parenteral cobalamin supplementation. Lancet. 1999;354:740741. PubMed
Sharabi, A., Cohen, E., Sulkes, J. and Garty, M. (2003), Replacement therapy for vitamin B12 deficiency: comparison between the sublingual and oral route. British Journal of Clinical Pharmacology, 56:635638. doi:10.1046/j.13652125.2003.01907.x BJCP
B12 also available as a nasal spray (www.nascobal.com),skin patch or mouth spray
B12 in a multivitamin may be counterproductive. The late renowned B12 researcher Victor Herbert determined that many multivitamin supplements also contain B12 analogs (meaning they prevent B12 absorption by interacting with them)
Herbert V. Vitamin B12. In: Ziegler EE, Filer LJ, eds. Present Knowledge in Nutrition. 7th ed. Washington D.C.: ILSI Press; 1996:191205.
Some good product choices:
Vegan B12 Sublingual Each melt-under-the-tongue tablet contains 1000mcg B12, also contains folic acid (400mcg) and B6 (2mg), all needed for MELATONIN production.
<$10 + s/h for 90 tablets (3 month supply). Also tastes good!
How much B12 to take?
| B12 Deficiency Replacement Doses | ||
|---|---|---|
| Oral or Sublingual (synthetic) | 1000 μg/day for 1- 4 weeks | |
| B12 Maintenance Dose | ||
| Food- cobalamin malabsorption | Perniceous anemia or No ileal receptors | |
| Oral or Sublingual (synthetic) | 125-500 μg/day | 1000 μg/day |
| Intramuscular (IM) | 1000 μg / month | |
VidalAlaball J, Butler CC, CanningsJohn R, et al. Oral vitamin B12versus intramuscular vitamin B12for vitamin B12deficiency. Cochrane Database Syst Rev, 2005;20;(3): CD004655.
Andres E, Loukili NH, Noel E, et al. Vitamin B12(cobalamin) deficiency in elderly patients. Can Med Assoc J, 2004;171(3):251259.
Oh RC, Brown DL. Vitamin B12deficiency. Am Fam Physician, 2003;1;67(5):979986
B12 doses to counter drug- induced malabsorption are undetermined
Since B12 is stored in the liver, it does not have to be supplemented every day. E.g. 1000 ug tablets can be taken every other day or every third day for lower dose requirements. In figuring your dose you will need to somewhat compensate for the finding that a singular higher dose is not as well absorbed as when split into smaller doses. The exact compensation has not been determined for all doses and conditions so you will need to experiment for your specific case. Unused B12 is eliminated from the body
Pernicious anemia and lack of ileal receptors requires the high 1000 μg dose that relies on the 1% passive diffusion of B12 at the terminal ileum a dose of 1000 μg would provide 100 μg B12 by this route without the need for gastric acid or intrinsic factor.
Painful IM B12 shots can be effectively replaced with HIGH oral doses that also rely on the 1% passive diffusion at the terminal ileum
B12 Toxicity?
No upper Intake Limit (UL) has been set for B12 – as there is little evidence of toxicity
Excess B12 is harmlessly eliminated
References
Liz da Silva Stacey McCray Vitamin B12: No One Should Be Without It. PRACTICAL GASTROENTEROLOGY ▪JANUARY 2009 Online Link
Linus Pauling Institute Online Link














