Aeberli I, Zimmermann M, Molinari L, et al. (2007) Fructose intake is a predictor of LDL particle size in overweight schoolchildren. Am J Clin Nutr.86:1174-1178. Pubmed
Bantle JP, Raatz SK, Thomas W, Georgopoulos A. (2000) Effects of dietary fructose on plasma lipids in healthy subjects. Am J Clin Nutr. 2000;72:1128-1134. Pubmed
Faeh D, Minehira K, Schwarz J-M, Periasami R, Seongsu P, Tappy L. (2005) Effect of fructose overfeeding and fish oil administration on hepatic de novo lipogenesis and insulin sensitivity in healthy men. Diabetes. 54:1907-1913. Pubmed
Hallfrisch J, Reiser S, Prather E. (1983) Blood lipid distribution of hyperinsulinemic men consuming three levels of fructose. Am J Clin Nutr:740-748. Pubmed
Havel PJ, Elliott S, Keim NL, Krauss RM, Teff K. (2003) Short-term and long-term consumption of high fructose, but not high glucose, diets increases postprandial triglycerides and apo-lipoprotein-B in women. J Invest Med.;52(suppl):S163. Google scholar
Kouvalainen K, Uhari M, Akerblom H, et al. (1982) Nutrient intake and blood lipids in children. Klin Padiatr. 194:307-309 Pubmed
Morrison J, Larsen R, Glatfelter L, et al. (1980) Interrelationships between nutrient intake and plasma lipids and lipoproteins in schoolchildren aged 6 to 19: The Princeton School District study. Pediatrics. 65:727-734 PubMed
Neuhouser ML, Tinker L, Shaw PA, et al. (2008) Use of recovery biomarkers to calibrate nutrient consumption self-reports in the Women’s Health Initiative. Am J Epidemiol. 167:1247-1259. PubMed
Osei K, Falko J, Bossetti B, Holland G. (1987) Metabolic effects of fructose as a natural sweetener in the physiologic meals of ambulatory obese patients with type II diabetes. Am J Med.;83:249-255. Pubmed
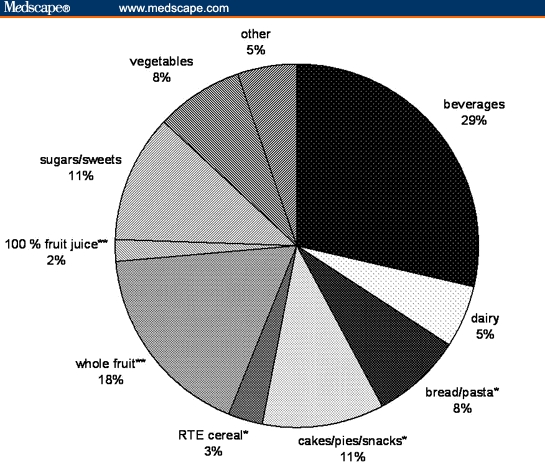
Park YK, Yetley EA, (Nov 1993) Review intakes and food sources of fructose in the United States. Am J Clin Nutr. 58(5 Suppl):737S-747S. PubMed
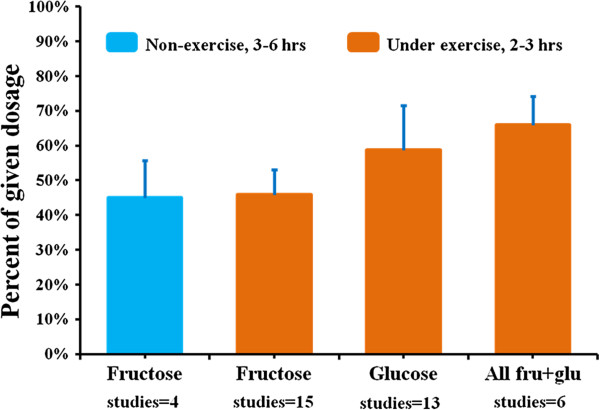
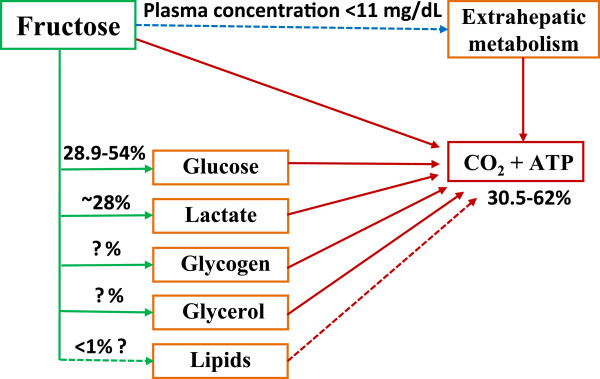
Sun, S. Z., & Empie, M. W. (2012). Fructose metabolism in humans – what isotopic tracer studies tell us. Nutrition & metabolism, 9(1), 89. PubMed
Teff KL, Elliott SS, Tschop MH, et al. (2004) Dietary fructose reduces circulating insulin and leptin, attenuates postprandial suppression of ghrelin, and increases triglycerides in women. J Clin Endocrinol Metab. 89:2963-2972. Pubmed
































 for Physical / Mental Health: Magnesium,
Omega-3 ,
C,
D,
Iodine in
“Make-it-Happen” smoothie
for Physical / Mental Health: Magnesium,
Omega-3 ,
C,
D,
Iodine in
“Make-it-Happen” smoothie 










{kind=link}