



$tatins - Don't save lives!
Statins supposedly prevent a high percentage of cardiovascular disease (CVD) - but they don't!
Statins are prescribed to prevent a significant amount of cardiac "events"
About 43 million adults in the U.S. (2019 data) are taking statin drugs (such as Pfizer’s Lipitor® (Atorvastatin calcium), Merk’s Zocor® (Simvastatin), AstraZeneca’s Crestor® (Rosuvastatin calcium), Pravachol® and Mevacor®) for the purpose of lowering blood cholesterol levels (by inhibiting an enzyme required for a rate-limiting step in the liver’s cholesterol production). They are taken as an attempt to prevent a significant number of “cardiac events”, such as heart attack or stroke, associated with problems seen in ischaemic cardiovascular disease (CVD), such as coronary heart disease, arrythmia, and high blood pressure.
However, pharmaceutical companies report misleading RELATIVE, not ABSOLUTE (REAL) risk reduction percentages
For example: Based on a specific trial involving over 10,000 people, Lipitor™ (atorvastatin) manufacturers claim a 36% RELATIVE risk reduction in heart attacks for people with risk factors for heart disease. However, this 36% figure does not take into account the number of people in the trial . . . 2% of people taking atorvastatin had heart attacks compared to 3.1% not taking atorvastatin. The manufacturer “take home” from these figures is that if you take their drug, you will have a RELATIVE risk reduction of ~36% (calculated as: (3.1-2.0) / 3.1 x 100 = 35.4%). However, the REAL risk reduction is only ~1% (3.1% compared to 2% ) – i.e. 1 out of a 100 people taking atorvastatin will be spared a heart attack – – – not so much of an attention-grabber is it? For more on this chicanery and to see some “REAL” risk reductions of taking statins:
Pharmaceutical companies report misleading RELATIVE, not ABSOLUTE (REAL) risk reduction percentages
To your detriment, statins DO significantly reduce cholesterol
However, it doesn’t follow that lowering cholesterol significantly decreases the risk of heart attacks or strokes:
- Multiple studies show that the cholesterol /heart disease connection is a myth. E.g. the large and ongoing Framington, Massachusetts population study found virtually no connection in CHD events with cholesterol levels in the 205-294 mg/dl range. Even extremely high (up to ~1200mg/dl) levels demonstrated trivial differences in CHD events. (Castelli, 1992; Smith & Pickney, 1991)
- 80% of people who develop CVD have the same blood cholesterol values as those who do not develop CVD or incur a heart attack.
High cholesterol DOES NOT CAUSE ischaemic CVD, such as heart attacks and strokes
Statins have an anti-inflammatory effect. Statins minimally protect people from heart attacks /stroke regardless of whether or not they have high levels of blood cholesterol or any other risk factors for that matter. i.e. the statins are having effects other than lowering cholesterol — in particular:
- Statins increase inflammation-controlling nitric oxide (NO) production in the vessel wall. Free radicals uncontrolled by sufficient antioxidants can diminish NO production, leading to atherosclerosis. Decreasing inflammation lowers the risk of heart attack and stroke.
But —–there are much better, natural ways than taking statin drugs to lower inflammation, without their multitude of undesirable side-effects.
For most people - Statins do NOT much reduce risk of heart attacks, strokes or mortality
However, taking statins can benefit those with familial hypercholesterolemia (FH). Individuals born with amilial hypercholesterolemia (FH) , a genetic disorder, are less responsive to the body’s usual measures of normalizing cholesterol. This group represents a minute fraction of those taking statins.
Statins as a SECONDARY prevention (those with established heart disease) reduce risk of a major coronary event ( e.g. heart attack or stroke) by 9% , but do not significantly reduce risk of death from other causes
Statin drugs were originally prescribed for secondary prevention. i.e. for those who already had established heart disease.
Real risk reductions of taking statins after either or both of angina or heart attack (Scandinavian 4S study, 1994. 4444 patients, median follow-up 1.9 years) :
- Major coronary events reduced by 9%. 622 out of 2223 patients (28%) in the placebo group and 431 out of 2221 (19%) in the simvastatin group had one or more major coronary events. A REAL risk reduction of 9%.
- Life expectation minimally increased. Coronary deaths: 189 out of 2223 (8.5%) in the placebo group and 111 out of 2221 (5%) in the simvastatin group a REAL risk reduction of 3.5%; while non-cardiovascular causes accounted for 49 out of 2223 (2.2%) and 46 out of 2221 (2.1%) deaths — a REAL risk reduction of 0.1%. (i.e. it saved one person out of a 1000 dying from other than cardiovascular causes). Study reported the 6-year probabilities of survival in the placebo and simvastatin groups at 87.6% and 91.3%, respectively. Again, not much between them!
- LDL cholesterol reduced. Patients taking Simvastatin had a 50% reduction in LDL cholesterol.
Real risk reductions of taking statins after either a ischemic stroke or TIA (brief episode of neurological function caused by loss of blood flow in the brain, spinal cord or retina, without tissue death). Meta-analysis examined 9 trials and 10741 patients with median follow-up period 2.5 years. (Tramacere et al, 2019)
- Ischemic stroke reduced 1.6%
- Ischemic stroke or TIA reduced 4.2%
- Cardiovascular event reduced 5.4%. A cardiovascular event defined as any sudden death, fatal or non-fatal acute coronary syndrome, stroke, intracranial hemorrhage, or pulmonary embolism; and rhabdomyolysis, myalgia, or rise in creatine kinase (CK).
- All-cause mortality not affected
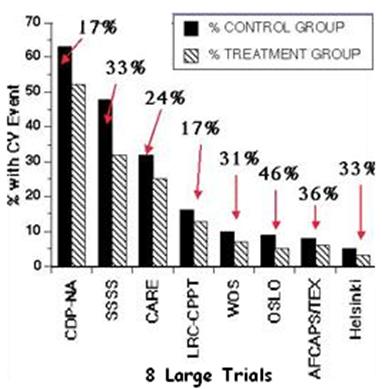
This chart shows the results of a meta-analysis of eight large worldwide trials (24,647 subjects WITHOUT established cardiovascular disease, average 73 years old, typically with a few risk factors for heart disease, such as high LDL, smoker, obesity, high blood pressure) comparing control groups to those of treatment groups lowering their cholesterol using statins. (Savarese G et al, 2013)
- Lowering cholesterol minimally reduced cardiac “events” and did not reduce risk of death. The people lowering their total cholesterol (particularly LDL cholesterol) levels, showed an average 39.4% RELATIVE risk reduction in number of heart attacks and 24.8% in strokes compared to the control groups. Sounds positive doesn’t it? — until you realize that:
(a) MI occurred in 2.7% of subjects allocated to statins compared with 3.9% of those taking placebo during a mean follow-up of 3.5 years. i.e. the REAL risk reduction was a mere 1.2%. i.e. Of 1000 people treated, only 12 would NOT have a heart attack.
(b) Stroke was reported in 2.1% subjects randomized to statins compared with 2.8% in placebo during a mean follow-up of 3.5 years. i.e. the REAL risk reduction was a mere 0.7%. i.e. Of 1000 people treated, only 7 would NOT have a stroke.
(c) The risk of all-cause death and CVD death were NOT significantly reduced.
- 65-75% of patients who lower their LDL cholesterol with a cholesterol-lowering therapy continue to have cardiovascular events.
Flawed “JUPITER Study” is the major supporting study in the push for statin use as a PRIMARY prevention against heart attack / stroke
(JUPITER: Justification for the Use of Statins in Prevention: an Intervention Trial Evaluating Rosuvastatin)
Headline: “Rosuvastatin can slash risk of heart attack by 54% and stroke by 48%”
“Rosuvastatin to prevent vascular events in men and women with elevated C-reactive protein”. This 2006 study published in the New England J. of Medicine in 2008 Ridker et al. 2008, supposedly determined that statin drugs could lower heart attack risk 54%, risk of stroke by 48%, and risk of needing angioplasty or bypass surgery by 46%, and the risk of death from all causes by 20%. It was taken at face value, despite the fact that funding for this study came from Astra-Zeneca, the maker of Crestor®.
The JUPITER trial promoted statin use as preventive medicine against a FIRST-time heart attack or stroke (i.e. primary prevention) adding to its original prescription for the prevention of a SECOND heart attack or stroke (i.e. secondary prevention), and so expanding the market to those with an inflammatory risk factor (elevated C-Reactive protein) for CVD. The study claimed that statins could significantly prevent people with elevated C-Reactive protein, but otherwise healthy without a history of cardiovascular disease (CVD) or high levels of low-density lipoprotein (LDL) cholesterol) from having a heart attack or stroke.
Lies, Damn Lies, Statistics — and the JUPITER study! :
In the JUPITER study there were 68 heart attacks in the placebo group and 31 heart attacks in the statin drug treatment group. A RELATIVE risk reduction of 54%. There were 64 strokes in the placebo group, compared to 33 strokes in the treatment group, a relative risk reduction of 48%. Sounds good, doesn’t it? However, here is the reality:
In a drug treatment group of 8,901 participants, the heart attack risk was reduced from a very low 0.76% to 0.35% and the risk of stroke from 0.72% to 0.37%. In effect, if you treat 300 people with expensive and dangerous drugs you might save one life. Under the best possible scenario, the real risk reduction was under 0.5%.
In perspective, consuming a handful of raw mixed nuts has a much higher real risk reduction!
Pharmaceutical companies report misleading RELATIVE, not ABSOLUTE (REAL) risk reduction percentages
Three articles were published in the Archives of Internal Medicine in June 2010, refuting the industry-funded JUPITER study claims
(1) An independent assessment of the same statistics in 2010 entitled “Cholesterol Lowering, Cardiovascular Diseases, and the Rosuvastatin-JUPITER Controversy. A Critical Reappraisal ” found that “the JUPITER Study” was severely flawed. This recent analysis did a careful and independent review of both results and methods used in the Jupiter Study and reported that the “trial was flawed”. In an unprecedented attack on the study they stated that “The possibility that bias entered the trial is particularly concerning because of the strong commercial interest in the study.”And concluded:
“The results of the trial do not support the use of statin treatment for primary prevention of cardiovascular diseases and raise troubling questions concerning the role of commercial sponsors.” (de Lorgeril et al, 2010)
(2) Meta-analysis of 11 randomized controlled trials (Ray KK et al, 2010). involving a combined total of 65,229 participants with a high-risk for heart disease and followed for approximately 244,000 person-years. No evidence was found to back up the JUPITER trial claim that statins can statistically reduce your risk of death when used as primary prevention against heart disease i.e. they don’t save lives even if you do have elevated risk factors. (Ray, K.K. et al, 2010).
(3) Cholesterol-lowering therapy for primary prevention: still much we don’t know. Dr. Lee Green of U. of Michigan Medical school points out that billions of revenue dollars were at stake for the study sponsor in the JUPITER trial, as well as potentially millions of dollars in royalties for the principal investigator. (Green LA, 2010)
$tatins are "pushed" mainly to make mega-profits for the drug companies
In 2008, Pfizer made $12.4 billion in sales of Lipitor® – the top-selling branded pharmaceutical in the world
Recommendations are an “Inside Job”. A panel of “experts” (8 out of 9 on the payroll of statin drug manufacturers) recommended lowering blood cholesterol of high-risk heart disease patients to levels so low, they are only attainable by using their employers’ statin drugs.
How many more studies do we need to show that statins don't work?
Studies by the Medical Research Council dating back to the late 1980s.
- Researchers found that of 1,000 men ranging in age from 35 to 64 who received treatment for mild hypertension over five years, there were six fewer strokes and two fewer cardiovascular events than would be expected. The REAL reduction was 0.9%. (Medical Research Council Working Party, 1985; Miall & Greenberg, 1987).
- 5 year study with 1000 middle-aged men having high cholesterol but no previous history of heart attack touted a 22% drop (relative risk, not real risk) in mortality. It resulted in 7 fewer deaths from cardiovascular causes, and 2 fewer deaths from other causes than would be expected. The real risk reduction was therefore a mere 0.9%. (9 out of a 1000 men ) The research was sponsored by Bristol-Myers Squibb Pharmaceutical (West of Scotland Coronary Prevention Study). (Shepherd et al, 1996).
The Heart Protection Study in the United Kingdom. 20,000+ participants aged 40 to 80 years with high risk of cardiovascular disease but average-to-low levels of total cholesterol and LDL cholesterol were treated with 40mg daily of simvastatin (Zocor®). 577 out of 10,269 people on statins and 701 out of 10,267 not treated died from a heart attack — a 25% relative risk reduction over five years, but a REAL risk reduction of only 1.7%. (Heart Protection Study Collaborative Group, 2002).
A study of 90,056 participants combining 14 randomised trials looked at the best outcome for people who had pre-existing conditions: 47% had pre-existing chronic heart disease, 21% had a history of diabetes and 55% a history of hypertension. The death rate was 8.5% among the statin group compared to 9.7% in the control group. This is a 1.2% REAL risk reduction. (Baigent C et al, 2005)
A 2008 study reported in the British Medical Journal – a meta-analysis of 10 randomized clinical trials of about 70,000 people followed for an average of four years. In these trials, people with risk factors for cardiovascular disease but no history of existing disease were randomized to receive statins or no treatment. The relative risk reduction was 12% for total mortality, 30% for coronary event and 19% for a cerebrovascular event (stroke). However, the real risk reduction was 0.6%, 1.3% and 0.4% respectively. The actual number needed to treat to save one life was 167. Despite this insignificant outcome, the authors of the study concluded, “In patients without established cardiovascular disease but with cardiovascular risk factors, statin use was associated with significantly improved survival and large reductions in the risk of major cardiovascular events.” The authors had significant associations with the drug companies. (Capewell, 2008).
Serious side-effects of statin drugs
Many body functions need cholesterol to function properly
The liver produces about 75% of the body’s cholesterol – because it needs it. Statin drugs (E.g. Lipitor® and Zocor®) work by arbitrarily inhibiting the enzyme HMG-CoA reductase used to synthesize cholesterol, reducing its availability for important functions:
- Cholesterol provides cell membrane integrity. An essential component of cell membranes (especially protective of nerve cells) ;
- Cholesterol is a precursor for vitamin D, stress and sex hormones
- Cholesterol is required for fat metabolism (being the raw material for making bile salts);
- Cholesterol is needed by brain serotonin receptors for emotional stability. Its deficiency is linked to depression, higher suicide risk and aggressive emotions /actions.
- With a cholesterol level in the blood of < 150 mg/dL your body is going to run short of supply. A more optimum blood cholesterol level is ~200 mg/dL.
There are many more reasons for having sufficient cholesterol:
Statins quench the "spark" needed for cellular energy production
CoQ10 is the “spark” that your cell mitochondria need to produce ATP energy molecules (the body’s energy “currency”) from your food and is also a major antioxidant in the body.
Statins block the body’s production of CoQ10. The inhibited enzyme HMG-CoA reductase is used to manufacture CoQ10. Passi S et al, 2003
Impaired mitochondrial function thus not only causes the body to produce less energy, but because CoQ10 is an antioxidant, it also increases levels of damaging free radicals in the mitochondria. The higher the statin dose and the longer duration of usage, the greater the effects on mitochondria.
Evidence links statin use with:
- Muscle pain/damage. The most common statin side effect is muscle pain felt as soreness, tiredness or weakness in your muscles; Various researchers estimate that ~1-8% of statin users will experience muscle pain and weakness as a side effect.
- Peripheral neuropathies (muscle damage outside the CNS (spinal cord and brain)). Symptoms include muscle weakness, numbness, tingling, pricking sensations, burning pain (especially at night) and/or sensitivity to touch. Left undiagnosed, neuropathy can lead to deterioration of the muscles and paralysis. This can affect throat muscles for swallowing, chest muscles for breathing, and let’s not forget that the heart is a muscle. A famous Danish study of neuropathy as a side effect to statin use concluded that a long-term user of statin drugs has a 4 -14 times greater risk of developing neuropathy than a person who does not take statin drugs.
- Rhabdomolysis. Rarely, statins can cause this life-threatening muscle damage (~ 1 case per 15 million prescriptions), which can cause liver damage, kidney failure and death. When muscle fibers break down, the body must eliminate the excess waste products. The waste products then overload the kidneys; apart from muscle pain, the other major symptom of rhabdomyolysis is dark, red, or cola colored urine;
“Converging evidence supports a mitochondrial foundation for muscle AEs (adverse effects) associated with statins, and both theoretical and empirical considerations suggest that mitochondrial dysfunction may also underlie many non-muscle statin AEs.
Evidence from RCTs (randomized controlled studies) and studies of other designs indicates existence of additional statin-associated AEs, such as cognitive loss, neuropathy, pancreatic and hepatic dysfunction, and sexual dysfunction“. American Journal of Cardiovascular Drugs, 2009
- Liver damage. Statins can cause your liver to increase its enzyme production; if the increase is significant and left to continue, this could lead to permanent liver damage. Concurrent use of other certain other cholesterol-lowering drugs, such as niacin, increase the risk of liver problems. In May 2000, the FDA warned about liver failure with regard to statin drugs.
- Tiredness. In mice experiments, administering statins lowered their ATP levels, and impaired energy metabolism.
- Statins can negate exercising benefits. in a 2013 Duke University medical center study Simvastatin attenuates increases in cardiorespiratory fitness and skeletal muscle mitochondrial content (higher content can beneficially increase cellular energy production) when combined with exercise training in overweight or obese patients at risk of metabolic syndrome.
37 overweight and sedentary participants (who had not exercised regularly for 12 months) with at least 2 metabolic syndrome symptoms such as high BP, excess abdominal fat and also somewhat elevated cholesterol levels were divided into two groups (a) Given 40 mg/day of Simvastin (Zocor) or (b) Received no medication. After 12 weeks of being supervised doing 45 minutes/day walking or jogging on a treadmill 5 days/week (and being instructed not to change their diet), the results were almost unbelievable. Micus et al, 2013
| Cardiorespiratory (aerobic) Fitness (average % change) | Skeletal muscle Mitochondrial content and enzyme activity (average % change) | |
|---|---|---|
| Unmedicated participants | Improved > 10% | 13% |
| Participants taking Zocor 40mg/day | 1.5% Some had reduced aerobic fitness | – 4.5% |
“Low aerobic fitness is one of the best predictors of premature death. And if statins prevent people from raising their fitness through exercise, then that is a concern.” – John P. Thyfault, senior author of study.
- Memory impairment, ALS, some psychiatric disturbances. Cognitive problems and memory loss are widely reported. Potential Effect of Statin Drugs on Pilot Performance
- Sexual dysfunction
- Cancer. Risk of cancer is significantly associated with lower achieved LDL-C levels, which low levels may in part offset any cardiovascular benefits. Alsheik Ali AA et al, 2007
If you insist on using statin drugs, you need to supplement CoQ10
Statin Producers Know that Statins Deplete CoQ10, but keep it hushed
Two U.S. patents describe a method for counteracting statin-associated myopathy and potential liver damage by concurrent administration of the statins with CoQ10. Although U.S. package inserts and marketing material do not mention the statins-CoQ10 link; both of these patents were assigned to Merck & Co. (manufacturer of Zocor). However, for 20 years, the producers of statin drugs have not acted upon this information and have failed to reveal the statin-CoQ10 connection to millions of statin users and to the medical community.
- Merck® patent prevents addition of CoQ10 to statin drugs. Since 1989, Merck has held US Patent No. 4,933,165 for the addition of CoQ10 to its anti-cholesterol drugs lovastatin (Mevacor), simvastatin (Zocor) and pravastatin, in order to counteract the side effects resulting from a dramatic CoQ10 deficiency in the human body. However, to date, Merck has not used this patent, which also prevents other companies from doing so.
- Another unused Merck®patent is blocking the use of CoQ10 for the purpose of counteracting liver damage. US Patent No. 4,929,437.
Canadian magazine advertisements for statins carry warnings of their effect on CoQ10 (ubiquinone) and Lp(a):
Vitamin C - God's Perfect Statin (without the negative side-effects)

Statin drugs inhibit the enzyme HMG-CoA reductase. This enzyme catalyzes the body’s manufacture of (1) cholesterol and (2) CoQ10
Vitamin C (Ascorbic acid) provides the human body a naturally controlled HMG-CoA reductase inhibitor (i.e. statin) :
When vitamin C levels are low. The body compensates and triggers HMG-CoA reductase activity ▲ to manufacture more cholesterol and ensure an adequate supply of “patch” material for arterial wall repairs; Also, more HMG-CoA reductase is available for CoQ10 production:
- HMG-CoA reductase▲ ==► CoQ10 production ▲
- HMG-CoA reductase▲ ==► Cholesterol production ▲
When vitamin C levels are high. HMG-CoA reductase activity is inhibited ▼, lowering cholesterol levels and CoQ10 production:
- HMG-CoA reductase▼ ==► CoQ10 production▼
- HMG-CoA reductase▼ ==► Cholesterol production▼
A significant difference between Vitamin C and statins is that Vitamin C modulates / controls CoQ10 production, whereas statins only inhibit its production
Sufficient (but not too high) Vitamin C actually promotes the production of HMG-CoA reductase and thus CoQ10.
CoQ10 is depleted when LDL cholesterol is oxidized during the plaque forming process. Harwood HJ et al, 1986
References
Alsheikh-Ali AA, Maddukuri PV, Han H, Karas RH. Effect of the magnitude of lipid lowering on risk of elevated liver enzymes, rhabdomyolysis, and cancer: insights from large randomized statin trials. J Am Coll Cardiol. 2007 Jul 31;50(5):409-18. doi: 10.1016/j.jacc.2007.02.073. Epub 2007 Jul 16. PMID: 17662392.
Baigent C et al (2005 Oct 8) Efficacy and safety of cholesterol-lowering treatment: prospective meta-analysis of data from 90,056 participants in 14 randomised trials of statins. Lancet. 366(9493):1267-78. Epub 2005 Sep 27. LInk
Capewell, S. (2008). “Will screening individuals at high risk of cardiovascular events deliver large benefits? No.” British Medical Journal 337: a1395.
Castelli, William (July 1992), “Concerning the Possibility of a Nat. . .” Archives of Internal Medicine, 152: (7): 1371-1372
de Lorgeril M et al (2010), Cholesterol lowering, cardiovascular diseases, and the rosuvastatin-JUPITER controversy: a critical reappraisal, Laboratoire Coeur and Nutrition, Faculty of Medicine, Université Joseph Fourier and Centre National de Recherche Scientifique, Grenoble, France, Arch Intern Med. 2010 Jun 28;170(12):1032-6 Link
Green LA (2010 Jun 28) Cholesterol-lowering therapy for primary prevention: still much we don’t know, Arch Intern Med;170(12):1007-8; Link
Harwood HJ et al, 1986, Inhibition of human leukocyte 3-hydroxy-3-methylglutaryl coenzyme A reductase activity by ascorbic acid. An effect mediated by the free radical monodehydroascorbate
Heart Protection Study Collaborative Group (2002). “MRC/BHF Heart Protection Study of cholesterol lowering with simvastatin in 20,536 high-risk individuals: A randomised placebo-controlled trial.” Lancet 360: 7-22.
Medical Research Council Working Party (1985). “MRC trial of treatment of mild hypertension: principal results.” British Medical Journal 291: 97-104.
Miall, W.E. and G. Greenberg (1987). Mild Hypertension: Is There Pressure to Treat? An account of the MRC trial. New York, Cambridge University Press.
Mikus CR,Boyle LJ,Borengasser SJ, Oberlin DJ, Naples SP,Fletcher J,Meers GM,Ruebel M, Laughlin MH, Dellsperger KC, Fadel PJ, Thyfault JP. Simvastatin impairs exercise training adaptations. J Am Coll Cardiol. 2013 Apr 10. pii: S0735-1097(13)01403-4. doi: 10.1016/j.jacc.2013.02.074. [Epub ahead of print] PubMed
Passi S et al, Statins lower plasma and lymphocyte ubiquinol/ubiquinone without affecting other antioxidants and PUFA, 2003
Ray KK, et al (2010) Statins and all-cause mortality in high-risk primary prevention: a meta-analysis of 11 randomized controlled trials involving 65,229 participants, Department of Public Health and Primary Care, University of Cambridge, Cambridge, England, Arch Intern Med. 2010 Jun 28;170(12):1024-31 Link
Ridker, P.M., E. Danielson, et al. (2008). “Rosuvastatin to prevent vascular events in men and women with elevated C-reactive protein.” New England Journal of Medicine 359(21): 2195-2207. Link to the JUPITER trial
Ridker PM; Jupiter Study, Group (Nov. 2003). “Rosuvastatin in the primary prevention of cardiovascular disease among patients with low levels of low-density lipoprotein cholesterol and elevated high-sensitivity C-reactive protein: rationale and design of the JUPITER trial” Circulation. 108 (19): 2292-7 Link
Savarese G et al (2013 Dec 3) Benefits of statins in elderly subjects without established cardiovascular disease: a meta-analysis. J Am Coll Cardiol;62(22):2090-9. doi: 10.1016/j.jacc.2013.07.069. Epub 2013 Aug 28. Link
Scandinavian 4S study (1994 Nov 19) Randomised trial of cholesterol lowering in 4444 patients with coronary heart disease: the Scandinavian Simvastatin Survival Study (4S) Lancet. 344(8934):1383-9. Link
Shepherd J et al. (1996). “Prevention of coronary heart disease with Pravastatin in men with hypercholesterolemia.” New England Journal of Medicine 333: 1301-1307.
Smith, R. and E.R. Pickney (1991) Diet, Blood, Cholesterol and Coronary Heart Disease: A Critical Review of the Literature, Vol 2, Vector Enterprises, Sherman Oaks, CA
Tramacere, I et al (2019) Comparison of statins for secondary prevention in patients with ischemic stroke or transient ischemic attack: a systematic review and network meta-analysis, BMCMedicine 17, Article number:67 Link










