Rajan S, Wallace JI, Beresford SA, et al. Screening for cobalamin deficiency in geriatric outpatients: prevalence and influence of synthetic cobalamin intake. J Am Geriatr Soc, 2002;50:624630.
B12 deficiency is commonly related to:
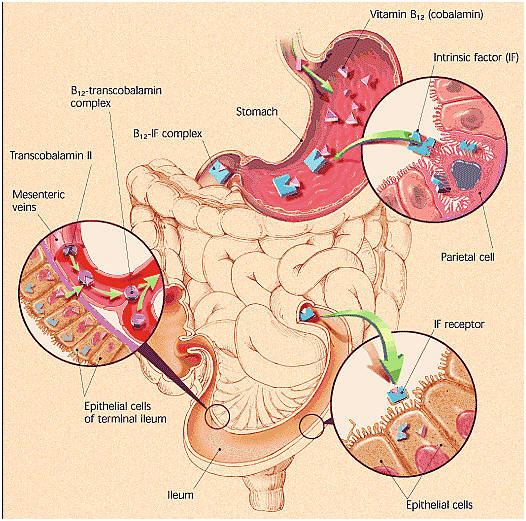
Food. Cobalamin malabsorption syndrome (MOST COMMON REASON) – occurs when the stomach lining loses the ability to produce intrinsic factor, a protein that binds to B12 to enable its absorption when it reaches the lower end of the small intestine.
- You can be consuming B12 in animal products and still not be absorbing enough of it
- Those over the age of 50 have limited ability to absorb B12
- Pernicious Anemia.
Progressive autoimmune destruction of stomach lining cells:
(1) Reduces secretion of B12– releasing gastric acid and enzymes
AND
(2) Antibodies bind to intrinsic factor preventing formation of B12– IF complex and consequently B12 absorption.
Intramuscular B12 shots are a common treatment, although high dose oral B12 delivers similar amounts (E.g. 1000mg supplies 1 mg B12 by passive absorption).
Kuzminski AM, Del Giacco EJ, Allen RH, Stabler SP, Lindenbaum J. Effective treatment of cobalamin deficiency with oral cobalamin. Blood. 1998;92(4):11911198. PubMed
Lederle FA. Oral cobalamin for pernicious anemia. Medicine’s best kept secret? JAMA. 1991;265(1):94-95.
Hathcock JN, Troendle GJ. Oral cobalamin for treatment of pernicious anemia? JAMA. 1991;265(1):96-97.
Food-bound vitamin B12 malabsorption. More common in those over 60 commonly resulting from atrophic gastritis, in which atrophy of stomach glands results in stomach inflammation (possibly associated with H. Pylori) and decreased stomach acid production, and thus nonrelease of B12 from food. This is different to pernicious anemia because intrinsic factor is still available, which means that crystalline-form B12 in supplements or fortified food, which is not bound to protein, can still be absorbed.
Aging. Typically, because of dietary insufficiency or malabsorption. Hydrochloric acid (HCl) is needed to release B12 from food, but HCl production decreases with age and HCl levels are decreased by long-term use of antacids or anti-ulcer drugs.
20- 50% of those over 50 are unable to absorb natural (protein-bound) B12. Institute of Medicine. Dietary reference intakes for thiamin, riboflavin, niacin, vitamin B6, folate, vitamin B12, pantothenic acid, biotin and choline. Washington, DC: National Academy Press 1998.
AIDS. Increases risk of B12 deficiency, possibly due to failure of IF-B12 receptors to take up IF-B12 complex. Shane B. Folic acid, vitamin B12, and vitamin B6. In: Stipanuk M, ed. Biochemical and Physiological Aspects of Human Nutrition. Philadelphia: W.B. Saunders Co.; 2000:483518.
Vegan diet. Animal products are the prime B12 source; predominantly vegetarian cultures (E.g. India) have high B12 deficiency rates.
- Surgical resection of ileal intestine containing IF- B12 receptors
- Pancreatic insufficiencies of enzymes or calcium
- Those taking Metformin. May interfere with absorption of calcium, required for small intestine receptors to take up B12. Herbert V. Vitamin B12. In: Ziegler EE, Filer LJ, eds. Present Knowledge in Nutrition. 7th ed. Washington D.C.: ILSI Press; 1996:191205.
Symptoms of B12 deficiency include:
- Megaloblastic anemia. Diminished folate production, even in the presence of folate; a symptom of pernicious anemia; produces large, immature, hemoglobin-poor RBCs
- Neurological. Numbness / tingling in arms, or legs, difficulty walking, memory loss, disorientation, dementia, possibly due to megaloblastic anemia or nerve sheath damage.
- GI-related symptoms – sore tongue, loss of appetite, constipation
Some diseases associated with B12 deficiency
Reference: Linus Pauling Institute
- Cardiovascular Disease (CVD) related to elevated homocysteine levels
- Cancer related to deficiency of folate and its connection to DNA synthesis
- Neural tube defects. Possibly connected to folates role in reducing homocysteine, since increased risk of NTD is associated with elevated levels of homocysteine
- Alzheimer’s disease / Dementia. Possibly connected to B12‘s role in myelin sheath integrity
- Depression
































 for Physical / Mental Health: Magnesium,
Omega-3 ,
C,
D,
Iodine in
“Make-it-Happen” smoothie
for Physical / Mental Health: Magnesium,
Omega-3 ,
C,
D,
Iodine in
“Make-it-Happen” smoothie 
























{kind=link}